Appendix A: Sample WOC Nurse Position Description: Hospital (Acute Care)
Position Title: WOC Nurse
Department: Division of Nursing or Department of Patient Services
General Description
The hospital-based WOC nurse serves as a clinical resource and consultant for the acute and rehabilitative care of patients with selected disorders of the gastrointestinal, genitourinary, and integumentary systems such as acute and chronic wounds (eg, complex draining wounds, fistulae, pressure ulcers, vascular ulcers), ostomies, percutaneous tubes, and continence disorders. Professional responsibilities are carried out through direct patient care, clinical consultation, education, research, and administration.
Qualifications
- Education and experience
- BSN (required) or MS (preferred).
- Two to four years of recent, relevant nursing experience (preferred).
- Graduation from a WOCN-accredited wound, ostomy and continence (WOC) nursing education program, or satisfactory completion of an accredited program within 6 months after assuming the position.
- License and certification
- Current RN licensure.
- Current certification in tri-specialty (CWOCN) by the Wound, Ostomy and Continence Nursing Certification Board.
- Current certification in cardiopulmonary resuscitation.
General Duties and Responsibilities (this list is representative rather than inclusive)
- General duties/responsibilities
- Utilizes the nursing process when directing or delivering care to patients with WOC needs including assessment, diagnosis, outcomes identification, planning and implementation (eg, coordination of care delivery, health teaching and promotion, consultation), and evaluation.
- Utilizes and maintains current physical, psychosocial, clinical assessment, and therapeutic communication skills to determine individual patient needs and expected outcomes.
- Participates in committees or task forces related to wound, ostomy, and continence issues.
- Wound/skin care
- Provides consultation for individuals with altered skin integrity (eg, pressure ulcers, draining wounds, fistulae) to develop individualized plans of care and attain expected outcomes.
- Provides guidance to staff in implementing protocols to identify, control, or eliminate etiologic factors for skin breakdown, including selection of appropriate support surfaces.
- With a physician's order, provides appropriate debridement of devitalized tissue (eg, conservative sharp debridement, silver nitrate [AgNO3] cauterization of nonproliferative wound edges, hypergranulation tissue, or to control minor bleeding).
- Provides appropriate education to patients, caregivers, and staff regarding skin care, wound management, care of percutaneous tubes, and draining wound/fistulae management.
- Validates pressure ulcer data collection for nursing quality indicators (eg, pressure ulcers and restraint use).
- Ostomy care
- Provides pre- and postoperative education to patients (and their families) who are undergoing ostomy surgery, with consideration of the need for physical and psychological adaptation.
- Marks the stoma site preoperatively by determining the appropriate site for stoma placement with consideration of the patient's anatomical markings, physical capabilities, and lifestyle.
- Assesses the stoma and stoma functioning and initiates appropriate procedures for stoma care (eg, removes rod/sutures, measures/fits a pouching system, teaches care of stoma/peristomal skin and pouch).
- Provides appropriate educational information to patients, including postoperative and discharge instructions about care, referrals, and supply needs.
- Serves as a resource for patients after discharge through telephone consultation or outpatient services.
- Continence care
- Identifies risk factors for urinary or fecal continence disorders.
- Assesses patients with urinary and/or fecal continence disorders.
- Establishes an appropriate management program to include dietary and fluid management; bowel training or stimulated defecation program; bladder retraining, prompted voiding, or a scheduled voiding program; pelvic muscle reeducation without biofeedback; indwelling catheter management; recommendations regarding containment/absorptive products and devices and skin care; and education and counseling for patients/caregivers.
- Identifies patients requiring referral for assessment/management of complex urinary or fecal continence disorders.
- Education
- Participates in developing and implementing procedures and protocols, based on current national guidelines, to deliver care to patients with the following:
- Urinary or intestinal disorders resulting in the need for an ostomy.
- Conditions requiring wound management.
- Impaired or altered skin integrity.
- Urinary and/or fecal continence issues.
- Assists the nursing and medical staff in maintaining current knowledge and competence in WOC care by providing the following:
- Formal or informal continuing education programs.
- Clinical rounds.
- Lunch and learn sessions.
- Orientation sessions.
- Collaborative practice committees.
- Nursing councils.
- Attends continuing education programs related to WOC nursing to maintain current knowledge and skills.
- Research
- Collaborates with leadership and multidisciplinary clinical practice teams to establish protocols, which support best practices to achieve optimal clinical benefits for patients needing WOC care.
- Administrative duties
- Maintains and submits required activity and statistical reports to the appropriate department supervisor.
- Contributes to the selection of cost-effective supplies and equipment related to WOC care, which might need to be individualized for different units/departments.
Appendix B: Sample WOC Nurse Consultant/Clinical Expert Position Description: Hospital (Acute Care)
Position Title: WOC Nurse Consultant/Clinical Expert
Department: WOC Nursing
Clinical Ladder: Level IV
Supervisor: VP of Nursing and Clinical Services
Supervision Exercised: Autonomous
General Description
The WOC nurse functions as a consultant and expert clinical nurse to assess, plan, implement, evaluate, and reassess (as indicated) the care of patients with abdominal stomas, acute or chronic wounds (eg, draining wounds, fistulae, pressure ulcers), and/or continence disorders.
Qualifications
- Education and experience
- BSN (required) or MS (preferred).
- Graduation from a WOCN-accredited wound, ostomy and continence (WOC) nursing education program or satisfactory completion of an accredited program within 6 months after assuming the position.
- License and certification
- Current RN licensure.
- Current certification in tri-specialty (CWOCN) by the Wound, Ostomy and Continence Nursing Certification Board.
- Current certification in cardiopulmonary resuscitation.
General Work Requirements
- Normal work hours per day.
- Normally works 32 to 40 hours per week.
- Normal work hours are 8 AM to 4:30 PM, Monday to Friday, excluding recognized holidays.
- Mental demands
- Exceptional mental alertness is required.
- Must be able to make clinical decisions regarding individualized patient care plans and establish priorities to provide effective, efficient care.
- Working conditions
- Frequent use of body substance isolation and contact precautions.
- Contact with patients under a wide variety of circumstances.
- There is a high probability that unexpected situations will occur.
- Physical demands
- Must be able to meet basic physical requirements: frequent walking, standing, lifting, or bending.
Primary Duties and Responsibilities: The following statements describe the principal functions and duties of the job and are not to be considered a detailed description of all requirements inherent in the position.
- Demonstrates competence and knowledge in the assessment, diagnosis, planning, implementation, and evaluation of care for patients of all ages with WOC needs.
- Provides consultation for individuals with altered skin integrity (ie, pressure ulcers, draining wounds, fistulae) to develop an individualized plan of care and attain expected outcomes.
- Provides guidance to staff in implementing protocols to identify, control, or eliminate etiologic factors for skin breakdown, including selection of appropriate support surfaces.
- With a physician's order, provides appropriate debridement of devitalized tissue (eg, conservative sharp debridement, silver nitrate [AgNO3] cauterization of nonproliferative wound edges, hypergranulation tissue, or to control minor bleeding).
- Provides appropriate education to patients, caregivers, and staff regarding skin care, wound management, care of percutaneous tubes, and draining wound/fistulae management.
- Provides pre- and postoperative education to patients (and their families) who are undergoing ostomy surgery, with consideration of the need for physical and psychological adaptation.
- Marks the stoma site preoperatively by determining the appropriate site for stoma placement, with consideration of the patient's anatomical markings, physical capabilities, and lifestyle.
- Assesses the stoma and stoma functioning and recommends appropriate procedures for stoma care (eg, measures/fits a pouching system, teaches care of stoma/peristomal skin and pouch).
- Assesses patients with urinary and/or fecal continence disorders.
- Recommends an appropriate management program to include dietary and fluid management; bowel training or stimulated defecation program; bladder retraining, prompted voiding, or a scheduled voiding program; pelvic muscle reeducation without biofeedback; indwelling catheter management; and recommendations regarding containment/absorptive products and devices and skin care.
- Provides education and counseling for patients/caregivers.
- Develops expected outcomes that reflect realistic, measurable, and patient-centered goals.
- Communicates the individualized plan of care to the interdisciplinary health care team and establishes criteria requiring reassessment or follow-up education.
- Participates in interdisciplinary collaboration to provide safe and therapeutically effective interventions across the continuum.
- Evaluates individual patient/family outcomes in response to the plan of care and the WOC nurse's clinical interventions.
- Provides outpatient services within the scope of WOC nursing practice (eg, stoma clinic, wound centers).
- Manages the WOC nurse's office and its operations.
- Provides guidance for the use of specialty support surfaces (eg, rental beds, chairs, lifts) and monitors for their appropriate use.
- Provides educational opportunities to update other health care professionals about current guidelines/standards of care for patients/populations with WOC needs or risks.
Additional Responsibilities/Duties
- Seeks opportunities for professional growth.
- Demonstrates and supports the organization's mission, values, and goals.
- Contributes to professional or consumer publications.
- Collaborates with community resources and organizations.
- Complies with reasonable requests to perform other duties.
- Maintains/demonstrates knowledge and skills to perform competently as required by the employer or state board of nursing (eg, conservative sharp debridement).
Appendix C: Sample WOC Nurse Consultant/Clinical Expert Position Description: Home Health
Position Title: WOC Nurse Consultant/Clinical Expert
Department: Home Care
Responsible to: Director of Nursing
General Description
The WOC nurse provides care in the home care setting to patients with acute or chronic wounds (eg, draining wounds, fistulae, pressure ulcers), ostomies, and continence disorders. Utilizing the nursing process, the WOC nurse provides hands-on care and educates clinicians, patients, and their families. The WOC nurse collaborates/coordinates care with nurses, the physician, and other health care team members to implement the plan of care and meet the rehabilitation needs for patients with wound, ostomy and continence (WOC) needs. Additionally, the WOC nurse performs other related tasks for documentation and supply management.
Qualifications
- Education and experience
- BSN (required).
- Graduation from a WOCN-accredited WOC nursing education program or satisfactory completion of an accredited program within 6 months after assuming the position.
- Two to 4 years of RN experience (preferred).
- License and certification
- Current RN licensure.
- Current certification in tri-specialty (CWOCN) by the Wound, Ostomy and Continence Nursing Certification Board.
- Current certification in cardiopulmonary resuscitation.
General Duties and Responsibilities (this list is representative rather than inclusive)
- Direct care
- Assists in caring for patients with stomas (eg, stoma site marking), acute or chronic wounds (eg, draining wounds, fistulas, pressure ulcers), and continence disorders.
- Initiates assessment, planning, and implementation of care for patients with WOC needs.
- Provides comprehensive postoperative care and education to patients with fecal or urinary diversions and their families.
- Evaluates, selects, and recommends supplies and equipment for patients with ostomies, acute or chronic wounds, and continence disorders.
- Consultation
- Serves as a consultant to the nursing staff, physicians, and other members of the health care team.
- Attends patient care conferences and staff meetings as needed and communicates patients' special needs to appropriate members of the health care team.
- Education
- Instructs nursing personnel in the care of patients with ostomies and acute or chronic wounds (eg, draining wounds, fistulas, pressure ulcers).
- Provides in-service educational programs as needed to staff, physicians, and other health care team members, in cooperation with the education coordinator to influence organizational best practices related to WOC nursing care.
- Maintains current knowledge and competence in WOC specialty nursing by participating in professional programs and organizations.
- Orients new nursing personnel and selected nursing students to the role of the WOC nurse.
- Research
- Develops and monitors standards of care and assists in the formulation and evaluation of procedures, protocols, and policies to maintain best practice.
- Engages in research, measurement of quality outcomes, and safety projects, as appropriate.
- Administration
- Evaluates, selects, and recommends supplies and equipment for patients with ostomies, draining wounds, fistulae, pressure ulcers, acute or chronic wounds, and continence disorders.
- Documents patient care in accordance with home health and nursing department policy.
- Performs other appropriately assigned duties, as required.
Appendix D: Sample WOC Nurse Position Description: Clinical Nurse Specialist
Position Title: WOC Clinical Nurse Specialist (AP-CNS)
Department: Nursing
Responsible to: Assistant Administrator for Nursing Services
General Description
The wound, ostomy and continence (WOC) clinical nurse specialist (CNS) demonstrates wound, ostomy, and continence professional activities that contribute to advancing the evidence and art of WOC specialty practice. The WOC CNS serves as a clinical resource for patients with wounds, ostomies, and continence disorders. Professional responsibilities are carried out through direct patient care, education, consultation, research, and administration.
Qualifications
- Education and experience
- Master's degree in nursing required.
- Graduation from a WOCN-accredited WOC nursing education program or satisfactory completion of an accredited program within 6 months after assuming the position.
- Three years of nursing practice.
- License and certification
- Current state license as an advance practice nurse (CNS, NP).
- Current certification in tri-specialty (CWOCN) by the Wound, Ostomy and Continence Nursing Certification Board.
- Current AP-CNS certification by American Nurses Credentialing Center.
General Duties and Responsibilities (this list is representative rather than inclusive)
- Clinical practice
- Provides comprehensive assessment of patients/situations.
- Initiates and interprets diagnostic tests and procedures as indicated.
- Provides direct care to selected patients.
- Determines diagnosis or nature of the problem.
- Identifies expected outcomes and plans individualized care to promote continuity across the continuum.
- Implements and coordinates plans for integrating systems and community resources.
- Assists in solving complex problems.
- Provides health education to selected patients and caregivers.
- Responds to changes in health care and safety initiatives.
- Consultation
- Integrates current evidence, clinical data, and information within theoretical frameworks when providing consultation.
- Evaluates the need for repeated consultations.
- Responds to identified needs of the health care team to enhance the work of others and effect change.
- Facilitates involvement of individuals and groups that have a direct interest in the situation or plan.
- Serves as a clinical consultant to committees (eg, safety, safe patient handling, infection control).
- Education
- Develops and implements educational programs for the health care team.
- Incorporates principles of teaching and learning in the planning, implementation, and evaluation of educational programs.
- Assists staff to identify learning needs.
- Participates in health education activities for the community.
- Serves as a role model to promote excellence by critical analysis of current research to expand clinical knowledge.
- Research
- Interprets, communicates, and incorporates current research findings and evidence-based guidelines into clinical practice.
- Conducts or contributes to nursing research.
- Identifies opportunities to mentor others in best practices to improve care processes.
- Administrator
- Provides leadership in the coordination and delivery of health care services across the continuum of care.
- Innovatively designs solutions to improve patient care, health services, and health outcomes related to WOC nursing care.
- Provides leadership in the development of care models for chronic issues related to WOC nursing care.
- Promotes clinical best practice standards as the basis for nursing practice.
Appendix E: Sample WOC Nurse Position Description: Nurse Practitioner in Adult Health
Position Title: WOC Nurse Practitioner in Adult Health (ANP)
Department: Patient Services
Responsible to: Director of Nursing Education, Director of Clinical Practice, or Medical Director of Primary Care
General Description
The WOC ANP functions as a generalist provider to the adult patient population with wounds, ostomies, or continence disorders, and functions in accordance with his/her State Nurse Practice Act. The wound, ostomy and continence (WOC) ANP has expert skills and is a leader in coordination of resources to facilitate achievement of health and wellness at an optimum level for each patient.
Qualifications
- Education and experience
- Successful completion of a recognized nurse practitioner program with a master's or doctor of nursing practice degree.
- Additional education in wound, ostomy, and continence nursing (required); graduation from a WOCN-accredited WOC nursing education program or satisfactory completion of an accredited program within 6 months after assuming the position (preferred).
- Minimum 2 years as an RN and 1 to 2 years as a nurse practitioner (preferred).
- License and certification
- Current state license as a nurse practitioner advance practice nurse.
- Current certification in tri-specialty (CWOCN) by the Wound, Ostomy and Continence Nursing Certification Board.
- Current NP certification by the appropriate national certifying body (eg, ANCC, AANP).
- Eligibility and acquisition of prescriptive privileges within 1 year (if required by practice).
Physical Requirements
- Physical requirements include those necessary to provide or influence patient care in the clinical setting (eg, ability to lift and/or move objects within job requirements, ability to stand for prolonged periods of time).
- Sensory requirements include the ability to articulate and comprehend the spoken and written English language (eg, acceptable vision and hearing).
General Duties and Responsibilities (this list is representative rather than inclusive)
- Assesses the physical and psychosocial status of clients via interview, health history, physical examination, and diagnostic tests.
- Interprets data, develops and implements therapeutic plans, and follows through on a continuum of client care across the health-illness spectrum and life span.
- Performs in accordance with organizational and work role performance standards. Tables 1 and 2 provide performance standards and related measurement criteria to meet organizational and work role requirements, respectively.
Table 1. Organizational Standards and Related Measurement Criteria
| Performance Standards |
Measurement Criteria |
- Responsibility: Acts responsibly as a member of the organization.
|
- Works independently, requesting assistance of the organization when needed.
- Anticipates problems and works to solve them.
- Performs duties willingly.
- Demonstrates appearance and hygiene appropriate to the delivery of quality service.
- Actively participates in all efforts to maintain a safe, clean environment.
- Recognizes that fulfilling the organization's mission involves successfully managing financial and other resources.
- Actively creates innovative, cost-effective systems throughout the organization to continuously improve the management of all resources.
|
- Sensitivity: Demonstrates sensitivity to customers' needs.
|
- Works collaboratively with other team members; treats other team members with consideration, courtesy, and respect, even in stressful situations.
- Continuously improves communication within the organization and with patients, visitors, and colleagues.
- Cooperates with other hospital departments.
- Encourages people to express ideas; encourages personal growth and learning for all; considers suggestions from other members of the team.
- Responds to patients, family members, hospital team members, and everyone else in a manner that indicates a desire to meet their needs and exceed their expectations.
|
- Accuracy: Demonstrates knowledge and attention to detail to ensure proper service to customers.
|
- Completes work in an accurate and thorough manner to ensure proper service to customers. Attention to detail is evident.
- Seeks information necessary for accurately completing job duties.
- Maintains current knowledge and skills necessary to perform competently.
|
- Timeliness: Recognizes time as the individual's most valuable resource.
|
- Responds promptly to customers' needs.
- Carries out work assignments within the allotted time.
|
- Ethics: Demonstrates a commitment to protecting the rights of customers.
|
- Discusses patient- and staff-related issues only in a confidential manner and setting, and only with those who have a right to know.
|
- Attendance: Maintains a satisfactory attendance record.
|
- Individual is in the disciplinary process with a minimum of a written warning.
- Individual has satisfactory attendance.
- Individual has perfect attendance.
|
Table 2. Work Role Performance Standards and Related Measurement Criteria
| Performance Standards |
Measurement Criteria |
- The ANP functions as an expert clinician in assessing, planning, evaluating, and revising care for the adult population.
|
- Provides direct care consistent with standards of practice by identifying, managing, or referring actual or potential problems of patients.
- Orders diagnostic and therapeutic interventions consistent with standards of practice.
- Demonstrates the ability to incorporate complex biopsychosocial dimensions into the nursing process at an advanced level.
- Demonstrates the knowledge and ability required to incorporate life span milestones into the nursing process (ie, age appropriateness, growth and development, aging).
- Collaborates with members of the health care team to facilitate coordinated delivery of care across the continuum.
- Requests consultation when specialized needs are identified.
- Utilizes prescriptive authority in a manner consistent with standards of practice.
|
- The ANP assumes a leadership role in implementing nursing practices to promote continuous quality improvement and desirable patient outcomes.
|
- Practices in accordance with current standards and research.
- Demonstrates continuous quality improvement in individual practice.
- Provides leadership to other nurses on the health care team in the use of research findings in current practice (eg, development of institutional standards and staff education).
- Participates in departmental and hospital efforts to continuously improve systems.
|
- The ANP demonstrates leadership in the development, implementation, and evaluation of community and patient education programs.
|
- Demonstrates an ability to provide individualized patient and family education related to health maintenance, illness, wellness, and prevention.
- Demonstrates knowledge of community needs and interests and develops creative, innovative mechanisms for meeting those needs.
- Provides leadership to other nurses on the health care team in the use of educational techniques.
|
- The ANP continually improves clinical avenues to provide optimal care while maximizing the use of resources.
|
- Participates in the attainment of budget objectives.
- Uses all information available to monitor use of resources, identify trends, and develop plans of action to ensure efficient practice.
- Maintains current knowledge of reimbursement issues as they apply to the ANP's individual practice.
- Seeks avenues for revenue generation in a creative, innovative, manner.
|
- The ANP creates an atmosphere for positive communication across all departments that plays a role in the continuum of care.
|
- Initiates or participates in team-building activities.
- Facilitates communication and collaboration among all members of the health care team.
|
- The ANP adheres to the policies and procedures outlined in the exposure-control plan regarding universal precautions; blood-borne pathogens; disposal of needles, syringes, and sharps; cleanup procedures for blood and body fluid spills; and storage, handling, and disposal of medical waste.
|
- Demonstrates knowledge and understanding in the policies and procedures outlined in the exposure-control plan.
- Practices safe work techniques and utilizes proper engineering controls to minimize the risk of blood-borne pathogen exposure.
|
- The ANP utilizes appropriate personal protective equipment when performing a task that presents a risk of exposure to blood-borne pathogens.
|
- Demonstrates knowledge of the appropriate level of personal protective equipment to be used in relation to a specific task.
- Degree of compliance is measured by personal observation by the immediate supervisor and managers and feedback from other supervisors and managers.
|
- The ANP adheres to hospital policies and procedures related to mandatory continuing education and annual health assessment.
|
- Completes annual records on mandatory continuing education assessment requirements and submits them to the human resources department.
- Completes annual health assessment form as required; maintains current inoculations.
- Submits the department-/state-required current license upon issuance or renewal to human resources.
|
Appendix F: Sample WOC Nurse Position Description: Independent Practice
Position Title: WOC Nurse Consultant
General Description
The independent WOC nurse, working under a contractual agreement between the nurse and the contracting organization, functions as a consultant for patients with complex draining wounds, fistulae, pressure ulcers, vascular ulcers, ostomies, and skin problems related to fecal and/or urinary continence disorders. The nurse is responsible and accountable for assessing, planning, implementing, and evaluating the care related to the aforementioned conditions.
Qualifications
- Education and experience
- BSN required or MSN (preferred).
- Graduation from a WOCN-accredited wound, ostomy and continence (WOC) nursing education program.
- Two to four years of relevant and recent experience as an RN (preferred).
- License and certification
- Current licensure as an RN.
- Current certification by the Wound, Ostomy and Continence Nursing Certification Board in one or more areas of WOC specialty nursing practice for the services to be provided (ie, tri-specialty [CWOCN], wound care nurse [CWCN], ostomy care nurse [COCN], continence care nurse [CCCN], or foot care nurse [CFCN]).
General Duties/Responsibilities (this list is representative rather than inclusive)
When developing a contract for independent practice, the WOC nurse should consider the following duties/responsibilities and specifically determine which services will be provided by the WOC nurse, and these should be delineated in the contract.
- Direct patient care: Serves as the primary patient educator for patients undergoing ostomy surgery who are referred to the WOC nurse.
- Provides preoperative visits and stoma site selection for elective procedures.
- Assesses, develops a plan of care for complicated pouching issues, and evaluates the outcomes.
- Provides education to patients and significant others regarding the care of the stoma and peristomal skin, and any special considerations that should be reported to the physician or the WOC nurse.
- Assists with selection and instruction of patients in the use of an appropriate pouching system and accessories, including where and how to obtain supplies.
- Determines if alterations in the pouching system are needed due to abdominal features, activity, adherence problems, diet, odor, or flatus and instructs patients/families and staff of those alterations.
- Coordinates discharge plans including follow-up visits with the WOC nurse as necessary and makes referrals for home health services if needed.
- Consultation
- Provides consultation for patients referred with complex draining wounds or fistulae.
- Selects and applies or recommends an appropriate system to contain drainage, recommends interventions to protect the surrounding skin, and provides the necessary instructions to the staff and the patient.
- Provides consultation for patients referred with or at risk for impaired skin integrity (eg, pressure ulcers, vascular ulcers, patients needing pressure redistribution devices).
- Recommends local wound care management.
- Recommends modalities to relieve or eliminate the cause(s) of the skin breakdown.
- Evaluates the progress or lack of progress toward wound healing and recommends changes in procedure or products as indicated.
- Provides consultation to patients referred with fecal and/or urinary continence disorder.
- Assesses the patient for the cause and type of continence disorders.
- Collaborates with the physician regarding the plan of care to control or manage continence disorders.
- Evaluates the patient's response to therapy and recommends alternative approaches as needed.
- Provides required instruction/education to the patient, family, and staff regarding concepts of bowel/bladder control.
- Provides in-service education to staff of the contracting facility.
- Provides education to staff regarding WOC care as agreed upon.
- Obtains CE approval for educational programs, when indicated and agreed upon.
Appendix G: Sample WOC Nurse Position Description: Industry
Position Title: Director of Professional Services
Responsible to: President, CEO, or Senior Vice President
General Description
The director of professional services shall assume responsibility for assisting the corporation in providing products and services in accordance with the corporate mission statement and philosophy. The director implements quality standards, develops educational programs and materials, and offers consultation to other members of the team in the area of clinical expertise.
Qualifications
- Education and experience
- BSN; master's degree from an accredited school of nursing preferred.
- Graduation from a WOCN-accredited wound, ostomy and continence nursing education program.
- Minimum of 2 to 4 years of experience as an RN preferred.
- Prior teaching, management, and leadership experience preferred.
- Working knowledge of quality management.
- License and certification
- Current RN licensure.
- Current certification by the Wound, Ostomy and Continence Nursing Certification Board in one or more areas of wound, ostomy and continence specialty nursing practice for the services to be provided.
General Duties and Responsibilities (this list is representative rather than inclusive)
- Develops, implements, and directs the corporation's quality assurance program in conjunction with input from senior operations personnel and develops a plan to introduce the program to the field.
- Defines the quality standards.
- Establishes a patient advocacy hotline and a patient evaluation response system.
- Develops a business plan that describes the structure, reporting mechanism, financial projections, and expected outcomes.
- Informs field centers of quality assurance standards as requested.
- Apprises senior operations personnel and local centers of regulatory guidelines promulgated by professional state practice associations (eg, Food and Drug Association, Department of Transportation, Compressed Gas Association). Establishes a monitoring mechanism to evaluate the center's regulatory compliance.
- Develops protocols and other collateral materials for review by senior management for home medical equipment centers to guide professional and patient care practices in home. Provides clinical/patient care consultation about the company's services, as required.
- Reviews client care and administrative policies and procedures encompassing the following:
- Intake procedures.
- Follow-up visit standards.
- Patient grievance procedures.
- Medical supervision procedures.
- Infection control guidelines.
- Monitors all product recall notices that affect field centers and notifies senior operations personnel and centers as appropriate regarding product recalls.
- Provides guidance to field home medical equipment centers regarding patient incidents. Assists in the investigative process as requested for incidents that may result in litigation. Serves as a liaison between the field centers and the corporate legal staff for all patient-/product-related incidents.
- Coordinates and networks with corporate and regional offices and departments to promote continuity and the efficient use of resources.
- Analyzes existing practices and provides recommendations as requested to senior and regional management regarding methods and procedures that facilitate integration of the corporation's spectrum of services, thus yielding improved service to patients, cost economies, and greater market penetration.
- Provides guidance to field home medical equipment centers and clinical staff in the provision of professional services. This includes supervision of performance evaluations, continuing education, and development of standardized procedures and practices.
- Assists senior management in the development of new programs as required, including the following:
- Analysis of needs.
- Development of a business plan.
- Assistance with program implementation.
- Production of collateral materials relating to professional and patient care practices for new programs.
- Provides consultation to field centers as requested regarding clinical and patient care issues and practices.
- Provides coordination of continuing educational offerings provided by the corporation to the community.
Appendix H: Sample Position Description: Certified Wound Care Nurse
Position Title: Certified Wound Care Nurse (CWCN)
Department: Nursing
Responsible to: Director of Nursing, Nurse Manager, or WOC Nurse Supervisor
General Description
The certified wound care nurse (CWCN) has the responsibility and accountability for utilizing the nursing process in the prevention and treatment of acute and chronic wounds throughout the organization. The CWCN functions primarily as a consultant providing direct patient care and education to selected patients and provides staff development in wound care.
Qualifications
- Education and experience
- BSN required.
- Graduation from a WOCN-accredited education program or specialty course, or satisfactory completion of program within 6 months of assuming new position.
- Minimum 2 to 4 years of RN experience preferred.
- License and certification
- Current RN licensure.
- Current certification in wound care nursing (CWCN) by the Wound, Ostomy and Continence Nursing Certification Board.
General Duties and Responsibilities (this list is representative rather than inclusive)
- Provides consultation and assistance to staff in developing and implementing protocols used in the identification and management of patients with potential or actual alteration in skin integrity.
- Provides guidance to staff in implementation of protocols to identify, control, or eliminate etiologic factors for skin breakdown, including selection of appropriate support surfaces.
- Establishes protocols and guidelines for appropriate and cost-effective use of therapeutic support surfaces.
- Evaluates the patient's response to treatment and the progress toward wound healing and makes adjustments and modifications in care as indicated.
- With a physician's order, provides appropriate debridement of devitalized tissue (eg, conservative sharp debridement, silver nitrate [AgNO3] cauterization of nonproliferative wound edges or hypertrophic granulation tissue, and to control minor bleeding).
- Provides consultation and assistance to staff in developing a plan of care to manage patients with draining wounds and fistulae (eg, containment of drainage and odor, protection of perifistular skin).
- Provides consultation and assistance to staff in developing a plan of care for patients with percutaneous tubes (ie, tube stabilization, site care, appropriate drainage collection system).
- Provides appropriate education to patients, caregivers, and staff regarding skin care, wound management, care of percutaneous tubes, and management of draining wounds/fistulae.
- Provides follow-up for patients with acute and chronic wounds (eg, draining wounds, fistulas) or percutaneous tubes through outpatient clinic visits and/or phone consultations.
- Initiates appropriate referrals for medical or surgical interventions.
- Assists staff to maintain current knowledge and competence in the areas of skin and wound care through orientation, regularly scheduled in-service programs, and by reviewing/updating policies and procedures according to national guidelines.
- Maintains records and statistics and submits reports to the employer.
- Analyzes stocked items and recommends appropriate additions and deletions to assure the quality and cost-effectiveness of products used for skin and wound care.
- Conducts product evaluations or contributes to research studies related to skin and wound care and submits reports and recommendations based on the results.
- Serves on systemwide committees and participates in systemwide projects as requested.
- Attends continuing education programs related to wound management.
Appendix I: Sample Position Description: Certified Ostomy Care Nurse
Position Title: Certified Ostomy Care Nurse (COCN)
Department: Nursing
Responsible to: Vice President/Director of Nursing, Nursing Manager or a WOC Nurse Supervisor
General Description
The certified ostomy care nurse has the responsibility and accountability for utilizing the nursing process in the management of patients with fecal and/or urinary ostomies throughout the organization. The certified ostomy care nurse functions primarily as a consultant providing direct patient care and education to selected patients and provides for ongoing staff development in ostomy care.
Qualifications
- Education and experience
- BSN required.
- Graduation from a WOCN-accredited wound, ostomy and continence (WOC) nursing education program or specialty course, or satisfactory completion of a program within 6 months of assuming new position.
- Minimum 2 to 4 years of RN experience preferred.
- License and certification
- Current RN licensure.
- Current certification in ostomy care nursing (COCN)by the Wound, Ostomy and Continence Nursing Certification Board.
General Duties and Responsibilities (this list is representative rather than inclusive)
- Provides consultation, direct care, and education to patients undergoing ostomy or continent diversion surgery.
- Visits patients preoperatively who are scheduled to undergo ostomy or continent diversion to provide informational, technical, and psychological support. Explains the surgical procedures and the rehabilitation process, selects and marks a potential stoma site, completes and charts the nursing assessment of the abdomen and psychological status.
- Initiates appropriate procedures for stoma care.
- Assesses the stoma and stoma functioning and alerts the physician to any problems.
- Removes sutures and/or the support rod.
- Measures and fits the stoma with a pouching system. Selects and provides appropriate products for the patient based on knowledge of the type of stoma, skin sensitivities, body contours, and disease processes. Orders supplies as needed.
- Instructs and demonstrates to patients and/or significant others the correct procedures to care for the stoma, peristomal skin, pouching system, and intubation and irrigation techniques (if indicated).
- Explains the availability of supplies/equipment and procedures for reordering.
- Provides counseling and educational literature to patients and their significant others.
- Provides consultation and assistance to staff in developing a plan of care to manage patients with an ostomy or continent diversion.
- Coordinates counseling services for patients and makes appropriate referrals to psychiatry, dietetics, social services, occupational therapy, or others that may be recommended by the physician.
- Provides follow-up for patients with ostomies or continent diversions through outpatient clinic visits and/or phone consults and initiates appropriate referrals for medical or surgical intervention.
- Assists staff to maintain current knowledge and competence in the areas of ostomy and continent diversion care through orientation, regularly scheduled in-service programs, and by reviewing/updating policies and procedures according to national guidelines.
- Maintains records and statistics and submits reports to the employer.
- Analyzes stocked items and recommends appropriate additions and deletions to assure the quality and cost-effectiveness of the products used for ostomy and continent diversion care.
- Conducts product evaluations or contributes to research studies related to ostomy care and submits reports and recommendations based on results.
- Serves on systemwide committees and participates in systemwide projects as requested.
- Attends continuing education programs related to ostomy and continent diversion care.
Appendix J: Sample Position Description: Certified Continence Care Nurse
Position Title: Certified Continence Care Nurse (CCCN)
Department: Nursing
Responsible to: Vice President/Director of Nursing, Nurse Manager or a WOC Nurse Supervisor
General Description
The certified continence care nurse (CCCN) has the responsibility and accountability for utilizing the nursing process in the management and treatment of patients with fecal and urinary continence disorders throughout the organization. The CCCN functions primarily as a consultant providing direct patient care and education to selected patients and provides staff development in continence care.
Qualifications
- Education and experience
- BSN required.
- Graduation from a WOCN-accredited education program or specialty course, or satisfactory completion of program within 6 months of assuming new position.
- Minimum 2 to 4 years of experience as an RN, preferred.
- License and certification
- Current RN licensure.
- Current certification in continence care nursing (CCCN) by the Wound, Ostomy and Continence Nursing Certification Board.
General Duties and Responsibilities (this list is representative rather than inclusive)
- Identifies risk factors for urinary and/or fecal continence disorders.
- Assesses patients with urinary and/or fecal continence disorders. Assessment includes the relevant history, a focused physical examination, a record of bladder and bowel elimination and incontinent episodes, simple bedside cystometry, and identification of complicating factors.
- Establishes an appropriate management program to include dietary and fluid management; bowel training or stimulated defecation program; bladder retraining, prompted voiding, or a scheduled voiding program; pelvic muscle reeducation without biofeedback; indwelling catheter management; recommendations regarding containment/absorptive devices and skin care; and education and counseling for patients/caregivers.
- Identifies patients requiring referral for assessment/management of complex urinary or fecal continence disorders.
- Provides consultation and assistance to staff in developing and implementing plans and protocols to identify and manage patients with potential or actual fecal and/or urinary continence disorders.
- Evaluates the patient's response to treatment and the progress of the continence care program and makes adjustments and modifications to care as indicated.
- Provides follow-up for patients with fecal and/or urinary continence disorders through outpatient clinic visits and/or phone consults and initiates appropriate referrals for medical or surgical intervention as needed.
- Assists staff to maintain current knowledge and competence in the areas of skin care and continence care through orientation, regularly scheduled in-service programs, and by reviewing/updating policies and procedures according to national guidelines.
- Maintains records and statistics and submits reports to the employer.
- Analyzes stocked items and recommends appropriate additions and deletions to assure the quality and cost-effectiveness of the products used for continence management.
- Conducts product evaluations or contributes to research studies related to continence and submits reports and recommendations based on results.
- Serves on systemwide committees and participates in systemwide projects as requested.
- Attends continuing education programs related to continence management.
Advanced Continence Care Skills: The following additional care may be provided if the CCCN has advanced continence care skills.
- A comprehensive assessment that includes performing the following examinations as indicted:
- A detailed physical examination and evaluation for prolapse and urethral hypermobility.
- Complex multichannel urodynamic studies, with or without fluoroscopic imaging and anorectal manometry studies.
- Management/interventions including pelvic floor rehabilitation and reeducation via electrical stimulation and biofeedback and fitting and placement of vaginal pessaries.
Appendix K: Sample Position Description: Certified Foot Care Nurse
Position Title: Certified Foot Care Nurse (CFCN)
Department: Nursing
Responsible to: Vice President/Director of Nursing, Nurse Manager, or a WOC-FC Nursing Supervisor
General Description
The certified foot care nurse (CFCN) has the responsibility and accountability for utilizing the nursing process in the management and treatment of patients with selected foot and nail disorders throughout the organization in accordance with licensure and educational preparation. The CFCN functions primarily by providing direct patient care to selected patients with foot/nail care needs and provides staff development in foot, skin, and nail care.
Qualifications
- Education and experience
- BSN preferred.
- Graduation from a WOCN-accredited wound, ostomy and continence (WOC) nursing education program or specialty course that includes foot/nail care, didactic and clinical; or completion of a specific foot/nail care continuing education course that includes foot/nail care, didactic/clinical, under the supervision of a foot/nail care expert.
- Minimum 2 to 4 years of experience as an RN, preferred.
- License and certification
- Current RN licensure.
- Current certification as a foot care nurse (CFCN) by the Wound, Ostomy and Continence Nursing Certification Board.
General Duties and Responsibilities (this list is representative rather than inclusive)
Three levels of foot/nail care have been described as basic, level I; intermediate, level II; and advanced, level III (Kelechi & Luckacs, 1996). The levels of care are based on the level of need of the patient and the qualifications of the staff who provide the care, which can vary according to state licensing laws and specific agency policies. For example, some states require a physician's order for nail debridement, while others do not (Etnyre, Zarate-Abbott, Roehrick, & Farmer, 2011).
- Basic foot/nail care, level I & intermediate foot/nail care, level II
- Identifies risk factors for foot disorders or ulcerations.
- Assesses patients with identified risk factors or actual foot disorders for:
- Risk of ulceration.
- Risk of amputation.
- Mobility and the need for footwear or mobility aids.
- Quality-of-life issues related to foot pathology.
- Provides assistance to staff in developing and implementing protocols used in the identification and management of patients with actual/potential disorders of the feet.
- Provides hygiene, trims toenails, and debrides thick toenails, corns, and calluses of selected at-risk patients.
- Establishes an appropriate management and education program to include foot assessment, prevention of injuries, hygiene, and skin and nail care.
- Identifies patients requiring referral to other specialists for assessment/management of complex foot disorders or ulcerations.
- With a physician's order, initiates dressings and other therapies such as compression.
- Evaluates the patient's response to treatment and the progress of the foot care management program.
- Provides follow-up for patients with foot disorders through outpatient clinic visits and/or phone consultation.
- Assists staff to maintain basic current knowledge and competence in the areas of prevention and skin care of the feet and lower extremities.
- Maintains records and statistics and submits reports to the employer.
- Analyzes stocked items and recommend appropriate additions and deletions to assure the quality and cost-effectiveness of products used for foot/nail care.
- Conducts evaluations of the products that are used for foot/nail care.
- Serves on systemwide committees and participates in systemwide projects as requested.
- Attends continuing education programs related to foot/nail care.
Advanced foot/nail care, level III
If the CFCN has advanced foot/nail care skills based on licensure and educational preparation, in addition to the basic level I and intermediate level II care, the following advanced care can be provided:
- Provides prompt interventions for specific foot complications.
- Patient assessment and advanced care are performed and referrals made for diagnostic tests or specialty care.
- Patients are reassessed by the CFCN as indicated for foot complications at least 4 times annually.
- Makes referrals for patients with complications who need ongoing assessment or care in the community until the condition no longer warrants the services.
- Pares (ie, sharp debridement) corns and calluses (selected RNs with competency).
- Prescribes appropriate pharmacological treatments for selected disorders of the feet or lower extremities (APRN with prescriptive authority).
- Performs digital blocks and excises ingrown toenails (APRN).
References
Etnyre, A., Zarate-Abbott, P., Roehrick, L., & Farmer, S. (2011). The role of certified foot and nail care nurses in the prevention of lower extremity amputation. Journal of Wound, Ostomy and Continence Nursing, 38(3), 242–251. doi: 10.1097/WON.0b013e3182152e93.
Kelechi, T., & Lukacs, K. (1996). Foot care in the home: Nursing and agency responsibilities. Home Healthcare Nurse, 14(9), 721–731.
Appendix L: Sample Position Description: Wound Treatment Associate
Position Title: Wound Treatment Associate∗
Department: Nursing
Responsible to: Director of Nursing or WOC Nurse Supervisor
General Description
Under the direction of an advanced practice WOC nurse, specialty WOC nurse, and/or MD, the wound treatment associate is responsible for provision of routine skin care, identification of patients at risk for pressure ulcer development, implementation of prevention protocols for patients at risk for pressure ulcer development, and assisting with the provision of comprehensive wound care and monitoring for patients with skin tears, incontinence-associated dermatitis, dehisced incisions, pressure ulcers, and lower extremity ulcers.
Qualifications
- Education and experience.
- Minimum of diploma, associate degree, practical/vocational nurse education, or completed training as a military medic/corpsman.
- Two years of clinical experience in nursing.
- Strong interpersonal skills.
- License and certification
- Licensed RN, LPN/LVN or military medic/corpsman (no license required).
- Certificate of successful completion of a Wound, Ostomy and Continence Nurses Society–endorsed Wound Treatment Associate Education Program.
Duties and Responsibilities
- Collaborates with other team members to provide routine care that keeps skin healthy.
- Collaborates with other team members to identify patients at risk for pressure ulcer development and to provide appropriate preventive care using established protocols.
- Identifies patient at risk for skin tears and for incontinence-associated dermatitis and initiates appropriate preventive care.
- Collaborates with other team members to identify and address causative and contributing factors to skin breakdown.
- Collaborates with other team members to assess and address systemic factors affecting wound healing.
- Collaborates with other team members to provide ongoing and comprehensive assessment and documentation of wound status and progress in wound healing.
- Collaborates with other team members to select appropriate dressings and to maintain a physiologic environment for wound healing.
- Identifies patients who require referral to a wound specialist, vascular surgeon, or other specialist for any of the following issues: evaluation for deterioration or failure to progress, management of closed wound edges (epibole), instrumental debridement of necrotic tissue, and differential assessment and management of lower extremity ulcers.
- Performs the following procedures when ordered and appropriate:
- Applies compression wraps.
- Measures ankle brachial index.
- Obtains swab wound cultures.
- Provides or assists with appropriate education regarding skin and wound care to patients, families, and staff.
- Collaborates with other team members to maintain an appropriate inventory of products for skin and wound care.
- Participates in quality improvement programs.
∗ Note: Each nurse is accountable for practicing in accordance with the specific requirements of the licensing boards in the state(s) in which he/she practices. Job titles and specific role functions are determined by the employing organization and should be consistent with state board of nursing licensing regulations and requirements.
Appendix M: Sample WOC Nurse Performance Appraisal: Acute Care
Date: _________
Employee Signature: ________________
Manager Signature: _________________
Meets Clinical Nurse IV Maintenance Criteria
- □ Clinical ladder validation criteria submitted.
Knowledge/Education, Leadership/Management, Clinical Practice, Quality/Safety, Research/Innovation.
- □ Certifications current: ______________________________
Completes annual required RN education
- □ Documented on in-service record.
Demonstrates maintenance of required annual competencies (if applicable):
- □ Conservative sharp debridement.
- □ Other: _________________________
Assessment Rating Scale:1 □ 2 □ 3 □ 4 □ 5
(1 = below expectations; 3 = meets expectations; 5 = exceeds expectations)
| |
Score |
- Performs essential functions identified in the position description.
|
□ 1 □ 2 □ 3 □ 4 □ 5 |
- Demonstrates organizational values in the work environment.
|
□ 1 □ 2 □ 3 □ 4 □ 5 |
- Performs essential functions to maintain a safe environment of care.
|
□ 1 □ 2 □ 3 □ 4 □ 5 |
Manager/Supervisor Comments:______________________________________________________________________
______________________________________________________________________________________________
______________________________________________________________________________________________
Employee Comments:_____________________________________________________________________________
______________________________________________________________________________________________
______________________________________________________________________________________________
Appendix N: Sample WOC Nurse Practitioner Performance Appraisal Form
Job Title: Nurse Practitioner
Department: Patient services
Job Criteria and Performance Standards
Scoring: Each performance standard scored on a scale of 1 to 5 (1 = below expectations; 3 = meets expectations; 5 = exceeds expectations).
Criterion 1: Provides diagnosis and treatment of common acute illnesses, prevention and maintenance health care to patients with stable chronic illnesses, and performs interim physical examinations for healthy patients within practice guidelines.
| 1. Performance Standards |
Score |
| 1.1. Elicits appropriate present and past medical history and reviews systems. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
| 1.2. Performs appropriate physical examination and orders appropriate diagnostic studies. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
| 1.3. Discriminates between normal and abnormal findings in history and physical. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
| 1.4. Establishes appropriate differential diagnosis. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
| 1.5. Assesses stability of chronic illness and compliance with present therapy and monitors for complications of disease or therapy. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
| 1.6. Establishes appropriate treatment plan. Assesses need for hospitalization or physician intervention. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
| 1.7. Determines timing for follow-up and orders appropriate referrals. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
1.8. Counsels regarding health maintenance and disease prevention and provides anticipatory guidance as appropriate.
Exceeds Standard
1.9. Demonstrates high degree of effectiveness in fulfilling standard as observed by supervisor. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
Comments:_____________________________________________________________________________________
_______________________________________________________________________________________________
Criterion 2: Provides health education to patients about ways to improve, promote, and maintain health status, including but not limited to providing educational information on disease/disease processes, self-care practices, and positive lifestyle choices (eg, diabetes, safe sex, weight loss, and smoking cessation).
| 2. Performance Standards |
Score |
| 2.1. Assesses learning capabilities and readiness of population or individuals and tailors education to meet age, developmental, and educational needs. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
| 2.2. Prioritizes learning needs and documents them accordingly. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
| 2.3. Ensures that time frame and subject matter are appropriate for target audience/individual. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
| 2.4. Utilizes appropriate teaching materials (eg, handouts, audiovisuals, demonstration) and documents use and patient outcome. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
2.5. Initiates, designs, and completes educational programs for patients, families, and targeted audiences.
Exceeds Standard
2.6. Demonstrates high degree of effectiveness in fulfilling standard as observed by supervisor. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
Comments:_____________________________________________________________________________________
_______________________________________________________________________________________________
Criterion 3: Maintains accurate records, medication lists, and documentation of care and follow-up for administrative purposes and reimbursement of services.
| 3. Performance Standards |
Score |
| 3.1. Adheres to agreed-upon format/protocol for documentation of records. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
| 3.2. Maintains appropriate level of documentation to promote/support level of complexity when compared against/to service fee charges. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
| 3.3. Reviews and updates problem list at least on annual visit/episodic visit by patient and initiates problem and medication lists for new patients. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
| 3.4. Documents telephone calls with patients and specialists. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
3.5. Documents visit in concise, clear, logical, and legible manner.
Exceeds Standard
3.6. Demonstrates high degree of effectiveness in fulfilling standard as observed by supervisor. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
Comments:_____________________________________________________________________________________
_______________________________________________________________________________________________
Criterion 4: Maintains competence in clinical practice.
| 4. Performance Standards |
Score |
| 4.1. Identifies the knowledge and skills needed through self-assessment, peer review, and supervisory review. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
| 4.2. Participates in a variety of educational activities in order to maintain and increase competency. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
| 4.3. Maintains licensure/certification. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
| 4.4. Uses continuing education opportunities as a basis for expanding knowledge and improving clinical skills and incorporates these into the daily practice. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
4.5. Participates in developing, implementing, and interpreting quality assurance/risk management programs.
Exceeds Standard
4.6. Demonstrates high degree of effectiveness in fulfilling standard as observed by supervisor. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
Comments:_____________________________________________________________________________________
_______________________________________________________________________________________________
Criterion 5: Supervises and intervenes with clinical issues and supports/directs triage by clinical staff when necessary. Implements clinical education and training of clinical staff when necessary.
| 5. Performance Standards |
Score |
| 5.1. Provides constructive feedback as it relates to performance, patient flow, and patient care issues. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
| 5.2. Provides in-services and clinical education for staff members on an “as-needed” basis. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
| 5.3. Is available for feedback on call back and triage issues as needed. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
| 5.4. Identifies barriers to patient care flow or delivery and assists at formulating corrective action. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
| 5.5. Serves as a role model for patient interaction and conflict resolution for clinical staff. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
5.6. Works collaboratively with health team members, both in and out of office setting, to ensure continuity of care and complete delivery of prescribed care.
Exceeds Standard
5.7. Demonstrates high degree of effectiveness in fulfilling standard as observed by supervisor. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
Comments:_____________________________________________________________________________________
_______________________________________________________________________________________________
Criterion 6: Adheres to the drug formulary developed by the practice.
| 6. Performance Standards |
Score |
| 6.1. Prescribes within the nurse practitioner scope of practice for state/licensing body. |
□ 1 □ 2 □ 3 □ N/A |
| 6.2. Ensures updated and accurate practice agreement as set forth in rules and regulations for licensing authority. |
□ 1 □ 2 □ 3 □ N/A |
Comments:_____________________________________________________________________________________
_______________________________________________________________________________________________
Criterion 7: Demonstrates regard for the dignity and respect for all patients, families, guests, and representatives of other organizations as well as fellow employees, volunteers, and medical staff in support of the practice's mission to provide consistent, quality health care services in a professional, caring, and responsive environment.
| 7. Performance Standards |
Score |
| 7.1. Maintains confidentiality of patient and of patient/practice information with no infractions. |
□ 1 □ 2 □ 3 □ N/A |
7.2. Consistently displays a caring and responsible attitude, represents the practice in a positive manner, and conducts all activities respecting patient/customer rights and expectations.
Exceeds Standard
7.3. Consistently makes extra efforts to achieve patient/customer expectations while discharging job responsibilities. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
| 7.4. Regularly maintains a neat appearance and adheres to department/corporation expectations for dress, including the wearing of appropriate identification. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
7.5. Interpersonal relations with other health care workers are regularly fostered in a courteous and friendly manner as evidenced by supervisory observation and peer input.
Exceeds Standard
7.6. The employee continuously exhibits self-initiated behaviors as outlined previously. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
| 7.7. Resolves conflicts with staff members by following established communication norms with limited involvement by supervisor to initiate resolution. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
| 7.8. Consistently receives and gives suggestions and constructive criticism in a professional manner. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
Comments:_____________________________________________________________________________________
_______________________________________________________________________________________________
Criterion 8: Demonstrates responsibility for individual performance and efficient utilization of products, supplies, equipment, and time to ensure the timely completion of duties and to promote financial viability through provision of services at a reasonable cost.
| 8. Performance Standards |
Score |
| 8.1. Maintains consistent level of productivity as influenced by impinging factors of access, practice load, and complexity of care. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
| 8.2. Performs other support functions to enhance the workflow. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
| 8.3. Provides proper notification for all absences or tardiness, scheduled shift, and scheduled time off in accordance with company policy. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
8.4. Consistently uses products, supplies, and equipment in an efficient manner, keeping waste within practice limits as observed by peers and administration.
Exceeds Standard
8.5. Regularly exceeds company standards and regularly suggests more efficient ways to complete tasks. |
□ 1 □ 2 □ 3 □ N/A |
Comments:_____________________________________________________________________________________
_______________________________________________________________________________________________
Criterion 9: Employee follows established safety precautions and procedures in the performance of all duties to ensure a safe environment.
| 9. Performance Standards |
Score |
| 9.1. Regularly performs job tasks in accordance with company policy and procedures, including appropriate use of equipment and machines and appropriate use in wearing of personal protective equipment and safety equipment. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
| 9.2. Demonstrates a complete knowledge of body mechanics by consistent use in the work setting as evidenced by no injuries sustained as a result of improper body mechanics in the evaluation period. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
9.3. Demonstrates a concern for cleanliness of self and work area and practices proper infection control and universal precautions techniques.
Exceeds Standard
9.4. No observable variances during the review period. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
| 9.5. Responds to codes in accordance with emergency procedures. |
□ 1 □ 2 □ 3 □ N/A |
| 9.6. Regularly maintains work area and equipment in a neat and orderly manner, assists in the cleaning of other work areas, and corrects any malfunctioning equipment or environmental conditions as observed by administration. |
□ 1 □ 2 □ 3 □ 4 □ 5 |
Comments:_____________________________________________________________________________________
_______________________________________________________________________________________________
Smart Goals
Goal and Target Date
- Goal: ___________________________________________________________________________
- Date: _________________________
- Goal: ___________________________________________________________________________
- Date: _________________________
- Goal: ___________________________________________________________________________
- Date: _________________________
- Goal: ___________________________________________________________________________
- Date: _________________________
Employee Name: _____________________________________________________________________
Employee Signature: _________________________________________________________________
Department Director/Supervisor Name: __________________________________________________
Department Director/Supervisor Signature:_______________________________________________
Date: _________________________
Date Issued/Approved: _________________________
Appendix O: Sample Structured Orientation Plan and Skills Checklist
Overview
The purpose of this form is to document completion of the orientation process and demonstration of skills in the critical components of wound, ostomy and continence nursing care. This form can be adapted with areas to place a checkoff or dates when the orientation/skills were completed. Additional skills or content areas can be added to meet the needs of the facility and/or the WOC nurse.
Utilization Guidelines
- Each nurse hired by the___________________ organization is assigned to receive 1 full day of orientation with the WOC nurse(s).
- The WOC nurse will utilize the Structured Orientation and Skills Checklist to ensure that:
- Critical procedures are reviewed and demonstrated to the orienting nurse.
- The orienting nurse is able to satisfactorily describe/demonstrate the critical skills.
- Following orientation to the WOC nurse role and the critical procedures, the skills checklist form will be completed by the WOC nurse with the following distribution:
- One copy to the orienting nurse's file.
- One copy to the orienting nurse.
- One copy to the appropriate supervisor.
- If the WOC nurse and the orienting nurse are unable to complete all of the components of the structured orientation, the appropriate supervisor will be notified and a follow-up plan will be established to complete the orientation and skills demonstration process.
Wound, Ostomy and Continence Care Orientation Guide and Skills Checklist
- WOC nurse role.
- Services provided/indications for referral.
- Referral process.
- WOC nurse and staff nurse roles and responsibilities.
- Wound care
- Critical assessment parameters:
- Identify location.
- Measure dimensions and depth in centimeters: length measured at longest head-to-toe dimension and width measured at widest point (side to side) perpendicular to the length; depth measured straight into wound at deepest point.
- Determine presence of sinus tracts and undermined areas: location and depth in centimeters.
- Stage pressure ulcers; classify other type of wounds as full/partial thickness.
- Assess status/appearance of wound bed (eg, granulating, necrotic, infected)
- Assess wound edges (open/closed).
- Assess exudate—volume, color, odor.
- Assess status of surrounding tissue (eg, intact, macerated, inflamed).
- Principles of management/dressing options.
- Importance of eliminating causative factors.
- Importance of providing nutritional support and glucose control.
- Guidelines for topical therapy.
- Options for wound with dry eschar.
- Options for superficial wound with minimal amounts of exudate.
- Options for superficial wounds with moderate to large amounts of exudate.
- Options for deep or tunneled wounds with minimal to moderate amounts of exudate.
- Options for deep or tunneled wounds with moderate to large amounts of exudate.
- Special considerations for leg ulcers.
- Importance of differential assessment and WOC nurse consult when needed.
- Venous ulcers: Importance of elevation and compression.
- Arterial ulcers: Issues regarding debridement and occlusion.
- Neuropathic ulcers: “Offloading” for plantar ulcers.
- Ostomy care.
- Pouch emptying.
- Indications and frequency.
- Guidelines for instruction to patient (eg, removing pouch clip, draining pouch, cleansing tail, reattaching clip).
- Pouch change: Fecal diversions.
- Guidelines for sizing pouch opening.
- Guidelines for cleansing and drying skin.
- Peristomal skin protection: Guidelines for paste application and use of skin sealants if needed.
- Procedure for centering and applying pouch.
- Pouch change: Urinary diversion.
- Guidelines for sizing pouch opening.
- Guidelines for cleansing and drying skin and for “wicking” the stoma.
- Peristomal skin protection: Guidelines for use of skin sealants, if needed.
- Procedure for centering and applying pouch.
- Management of peristomal skin breakdown
- “Crusting” procedure (eg, use of skin barrier powder and skin sealant).
- WOC nurse referral for severe or nonresponsive skin breakdown.
- Dietary/fluid modifications (teaching guidelines).
- Colostomy: No absolute restrictions, reduction or “timing” of gas-producing foods, fiber/fluids needed to prevent constipation.
- Ileostomy: Importance of increased fluid intake, cautious intake of high-fiber foods to prevent food blockage.
- Urinary diversion: Importance of adequate fluid intake.
- WOC nurse availability for bowel and bladder retraining/assistance with continence issues.
Appendix P: Sample Annual Conference Planning Time line
Suggested Time Frame and Actions to Be Taken: Starting 36 Months Prior to the Date of the Program.
36 Months in Advance
Form the Planning Committee
- For ANCC-accredited programs, the nurse planner coordinator is an RN (minimum BSN or master's prepared); members hold BSNs.
- Individuals with previous experience in planning seminars/programs are helpful.
- Persons who have expressed an interest in working on the planning committee and can commit to the expectations and responsibilities of a committee member are good choices.
- Meetings may need to be held quarterly the first 2 years and then monthly.
- Establish specific timetables for marketing and arranging convention center space.
- Assign areas of responsibilities to committee members.
- Members should provide general update to committee during regularly scheduled meetings.
30 Months in Advance
Site Selection/Negotiation
- Locale may have been predetermined by rotation schedule or committee selection based on prior sites, the time of year that the program has previously been held, and other activities that were identified as affecting attendance.
- Determine/compile preferred dates/sites.
- Determine/solicit facility availability and capabilities. Conduct site visit.
- Facility must be able to accommodate program schedule, meeting room needs (eg, general session vs breakouts), and the required exhibit space.
- Determine available room blocks and rates quoted (single or double).
- Determine audiovisual (AV) support, food function capabilities, handicap accessibility, and exhibitor table space, if required.
- Negotiate waiving meeting room rental based on food functions, complimentary rooms per number of reserved rooms per night, and special rates for faculty or committee members.
- Negotiate a “set” (confirmed) room rate—same rate housing 1 or 4 persons. Inspect the rooms.
- Establish method of room reservation and confirm if reservations should be made directly with the hotel or through a group.
- Present details of facility and contract to committee prior to commitment.
- Reserve site/dates—submit security deposit if required. Coordinator signs contract.
24 Months in Advance
Topic Selection/Objectives/Program Schedule/Evaluation
- Compile a needs assessment from prior program evaluations, questionnaires, or requests received from potential participants.
- Select theme and topics.
- Theme should have a central or specific focus.
- Verify target audience.
- Usually driven by topic selection; could be general health care, nursing, or specialty focus.
- Determine program schedule based on number of topics selected.
- Will the program all be general sessions or will breakout sessions be included, and on which days?
- Speaker solicitation/outlines.
- Determine speakers to address the selected topics who have recognized expertise in the field of the specific topic.
- Speakers who have been recommended or previously heard are preferable.
- Do not overlook nurses or local speakers, which can help contain costs.
Exhibitors
- Compile a list of exhibitors—consider previous participants. May need to develop criteria for selecting/admitting exhibitors based on topics presented at conference. For example, if a conference is planned only about continence disorders, having a significant number of bed companies will not support the focus of the conference.
- Determine fees—based on the number of days available for exhibitors and the space requirements of individual exhibitors (eg, a bed company usually requires more space than other vendors).
- Identify what the fee covers (ie, number of representatives per space, representatives attending educational/social/food functions) and include this expense in the fee.
- Consider a discount for early registration or a late fee if the registration deadline is missed.
- If the number of exhibit spaces is limited, stress early registration and stick to the deadline.
- At some meeting facilities, the fee for exhibit space is waived based on food and beverage expenses during the meeting.
- Exclusive viewing times for exhibits are recommended to ensure support from the solicited companies. Exhibit times that compete with educational or business sessions or that are scheduled for brief periods of time are usually not well attended and, therefore, are not believed to be beneficial for exhibitors.
- One- to 2-hour exhibit sessions are recommended.
- Serving refreshments in the exhibit hall during the exhibit sessions also helps draw attendees to the exhibit area.
- Early morning exhibit sessions usually are not well attended.
Registration/Budget Projections
- It is recommended that 1 person, ideally the treasurer, be responsible and accountable for all monies.
- Registrations from attendees should be sent to the designated person(s).
- Exhibitor's fees should be forwarded to designated individual/treasurer.
- Develop budgetary needs with input from each committee member regarding expenses that will be incurred from his or her area of responsibility.
- Determine the speakers' honoraria and what travel expenses will be reimbursed.
- Review menu items and determine a cost per person for food and beverage.
- Determine registration fees with committee input:
- Special rates might be developed for students, retirees, and more than 1 person attending from the same institution.
- Fees for daily walk-in registration and early or late registration also should be established.
- In setting the fee, consider the costs of the program for all food functions, costs for room rental, AV expenses, speaker fees, and any expected profit margin.
- Develop a cancellation policy and procedure.
18 Months in Advance
- Identify topic and audience, overview of desired content, honorarium, and expenses (ie, room, travel, meals) offered, length of presentation (consider need for question-and-answer period).
- Develop written behavioral objectives for the program and individual topics.
- Identify and invite possible speakers for selected topics.
- Outline speaker responsibilities, including honorarium and travel expenses.
- Negotiate any fees and confirm all of the speaker's information in writing. This should include expectations regarding the presentation, handouts, biography, presentation outline, AV needs, arrival and departure information, location of conference, and so forth.
- Request necessary American Nurses Credentialing Center (ANCC) forms from speakers.
- Invite potential exhibitors.
- Send invitation letters, which should include dates, location, the conference theme, program topics, exhibit times, and the fee structure plus what is included in the fee (eg, number of reps).
- A registration form should be completed by each company that plans to exhibit. It should include all information exhibitors need to provide, including a company description.
- Confirm receipt of exhibitors' fees. If you have a late fee structure in place, notify exhibitors if the fee has been received after the deadline.
- Confirmation letters to exhibitors should include a map or directions to the location of the meeting, instructions regarding shipping of booth materials, and setup and teardown times.
- Develop the brochure to send to potential program attendees.
- Consider layout, type of print, paper color and texture, content, registration information, hotel information (if applicable), map to location, food functions included, and special events.
- Contact printers and determine cost. Determine whether printer can provide mailing services.
- Utilize printer resources for design ideas.
- Determine sources of mailing lists based on the identified target audience.
- Approve the brochure design and confirm content and commence printing.
- Seek sponsorship for conference (usually the responsibility of the conference coordinator).
- Sponsorship is typically solicited for specific functions or activities such as:
- Speakers.
- Receptions.
- Conference items (eg, attendee bags, hotel key cards).
- Sponsorship requests should be made in writing, although phone contact is often beneficial because it is more personal and direct. Talking by phone also allows both parties to explore options and determine how the sponsorship can best benefit both parties.
- Appropriate acknowledgment of all sponsors should be provided in the program booklet along with appropriate signage.
- Sponsors of special events (either solely or jointly sponsored) should be acknowledged separately from supporters who contribute to the overall program or speakers' support.
12 Months in Advance
- Provide an outline of the program schedule and objectives, information about the fee structure, and the cancellation policy to the promotional chair/public relations committee for inclusion in the conference/program brochure.
- Procure commitments from speakers.
- Send a reminder to exhibitors who have not responded.
- Confirm sponsors.
6 Months in Advance
- Request the packet to apply for continuing education (CE) contact hours for the program from the accredited body that will approve the program for CE.
- Develop the evaluation tool based on the American Nurses Credentialing Center's Commission on Accreditation (ANCC) criteria or in accordance with the accredited approver's guideline. Included the evaluation tool in the conference booklet at the time of registration.
- Secure the needed written information to complete the CE application packet from speakers.
- Mail brochures.
- Note the early bird deadline (if relevant) and also the deadlines for the hotel registration, which are typically 1 month prior to the actual date of the conference.
- Develop the format for the program booklet to be distributed at registration.
- Cover might reflect theme or concept used in brochure.
- Content should include objectives, speakers' information, content outlines, bibliographies, schedule at a glance, committee members, posters, recognition of any sponsors/supporters, and so forth.
- Assemble program booklet and send to the printer.
- Determine and initiate registration strategies and financial records.
- Finalize program logistics.
- Arrange for necessary AV equipment, determine room assignments, arrange for moderators/monitors for each presentation, determine setup of rooms to maximize speaker visibility, determine lighting requirements for speakers using slides or overheads, and so forth.
- Based on information submitted by each speaker, determine the time, location, and type of AV equipment needed; submit requests to the AV company.
- Assign moderators to introduce speakers and inform them of their duties. Moderators should greet the speaker half an hour prior to the presentation; review introductory remarks (ie, speaker bio—how to introduce the speaker), assist with AV needs; escort the speaker to the room; and check the microphone, pointer, and lighting controls with the room monitor or AV personnel.
- Determine layout of the exhibit area. Avoid having “like” companies adjacent to one another, especially bed companies, if possible.
- Determine location for exhibitor registration, have name tags available, and provide each company with a list of preregistered attendees in its registration packet.
- Have appropriate signage made to indicate exhibitor registration and if desired, signage for each exhibitor at the conference.
- Be sure that exhibitors are in their designated space in the exhibit area and that they do not extend into adjacent spaces.
- Determine location for attendee registration and solicit volunteers to assist with registration, if needed.
5 Months in Advance
- Submit the completed application and fee for CE approval to the appropriate association that is an accredited approver of CE (eg, ANCC, State Nurses Associations).
- This may need to be done earlier based on the time line given to you by the accredited CE approver.
4 Months in Advance
- Monitor financial projections.
- Send confirmation to registrants.
2 Months in Advance
- Contact speakers to confirm dates, time, location, and other details related to presentation, transportation, or lodging.
- Plan the schedule/staff for the registration areas for exhibitors and participants.
- Verify exhibitors and the number of representatives designated to attend.
- Provide exhibitors with a registration packet, program booklet, and rules list for exhibitors.
- Notify the contact person for the exhibitor about the time of the exhibitors' meeting during conference, if applicable.
- Reconfirm details of the conference with the meeting facility and reconfirm commitments of committees to assist with on-site conference needs.
- Communicate the food and beverage orders directly to the catering manager at the facility.
- Any changes in food and beverage orders since first reviewed should be discussed.
- Review the number of anticipated attendees, being mindful of the allocation of space needed for food functions. Coffee by the gallon is more cost-effective than per person. Sodas or bottled waters should be purchased by usage (based on consumption) versus per person, if served during a break.
- If a food function is being solely funded by a specific sponsor, the caterer should be made aware of billing arrangements.
- Verify with the catering department all the required food services and the specific date that is required for final confirmation of the number of attendees to be served (ie, usually 3 days prior to the actual event); review any special food requirements.
- Confirm that all necessary forms and required information for CE, along with required payment, have been completed.
1 Month in Advance
- Prepare “certificate of attendance” forms. Include the approval number or appropriate information from the CE-accrediting body on the certificate.
- A certificate may be given for the total program, which requires the participant to attend the entire program, or separate certificates can be awarded for each day the participant attends. Follow the guidelines for determining and awarding CE, as identified by the accredited approver in the CE application packet.
1 Week Prior
- Finalize food and beverage requirements and your “guaranteed” numbers with the catering manager. Remember, you can always go up in your numbers, but once they have been guaranteed, you cannot reduce them.
At Conference
- Compile registration packets and have name tags made for attendees who have preregistered.
- Have appropriate signage made to indicate attendee registration area.
- Attendees to complete necessary registration information for roster of attendance.
- Greet speakers; confirm AV requirements.
- Provide additional evaluation forms at the conference.
- The conference coordinator should review food and beverage receipts with the caterer each day. Keep a copy of the receipts. You will receive a final bill after conference. Compare your receipts from the conference to the final bill that you receive.
End of Conference
- Collect the final evaluations; distribute certificates of attendance.
- Thank speakers; distribute honorariums.
- Submit bills to the treasurer or the treasurer's designee.
Postconference
- Collate evaluations and submit to conference coordinator.
- Send written acknowledgment to speakers and include evaluation summaries for individual presentations.
- Treasurer or designee facilitates payments after review of all invoices.
- Submit all necessary postconference information to the accredited CE approver as requested. This typically includes a roster of attendance, program evaluation summaries, and posttest results, if applicable. Check the accredited CE approver's guidelines for the specific information and deadlines for submitting the postconference information.
Appendix Q: Sample Conference Forms: Budget, Application for Exhibit Space, Exhibitor Evaluation, and Conference Evaluation
| |
Budget for Prior Year |
Actuals for Prior Year |
Current Year Budget |
Comments |
| Income |
|
|
|
|
| Exhibits |
$ – |
$ – |
$ – |
This column is important to complete. When you are determining a budget line item, please note how you arrived at that figure. |
| Registration |
$ – |
$ – |
$ – |
ie, registration income – 100 Members at $∗∗= $ and 50 Nonmembers at $50 = |
| Event Sponsorship |
$ – |
$ – |
$ – |
|
| Commercially Supported Symposia |
$ – |
$ – |
$ – |
|
| Unrestricted Educational Grant |
$ – |
$ – |
$ – |
|
| Postmeeting List Sales |
$ – |
$ – |
$ – |
|
| Total Income |
$ – |
$ – |
$ – |
|
| Expenses |
|
|
|
|
| Abstract Management |
$ – |
$ – |
$ – |
|
| CE Administration |
$ – |
$ – |
$ – |
|
| Marketing Annual Conference |
$ – |
$ – |
$ – |
|
| Audiovisual |
$ – |
$ – |
$ – |
|
| Audience Response Units |
$ – |
$ – |
$ – |
|
| Awards |
$ – |
$ – |
$ – |
|
| CD ROM |
$ – |
$ – |
$ – |
|
| Commercial Supported Symposia |
$ – |
$ – |
$ – |
|
| Decorator |
$ – |
$ – |
$ – |
|
| Disability Accommodations |
$ – |
$ – |
$ – |
|
| Equipment Rental |
$ – |
$ – |
$ – |
|
| Food and Beverage |
$ – |
$ – |
$ – |
|
| Gratuities |
$ – |
$ – |
$ – |
|
| Gifts/Amenities |
$ – |
$ – |
$ – |
|
| Insurance–Cancellation |
$ – |
$ – |
$ – |
|
| Meeting Space Rental |
|
|
|
|
| Membership Booth/Book Store |
$ – |
$ – |
$ – |
|
| Opening/Closing Speaker |
$ – |
$ – |
$ – |
|
| Photography |
$ – |
$ – |
$ – |
|
| Posters |
$ – |
$ – |
$ – |
|
| Printing |
$ – |
$ – |
$ – |
|
| Registration |
$ – |
$ – |
$ – |
|
| Shuttle Service |
$ – |
$ – |
$ – |
|
| Signs |
$ – |
$ – |
$ – |
|
| Speaker Honoraria |
$ – |
$ – |
$ – |
|
| Speaker Housing |
$ – |
$ – |
$ – |
|
| Speaker Per Diem |
$ – |
$ – |
$ – |
|
| Speaker Web site |
$ – |
$ – |
$ – |
|
| Speaker Travel |
$ – |
$ – |
$ – |
|
| Sponsored Items |
$ – |
$ – |
$ – |
|
| Supplies |
$ – |
$ – |
$ – |
|
| Total Direct Expense |
$ – |
$ – |
$ – |
|
| Copies |
$ – |
$ – |
$ – |
|
| Management Fees |
$ – |
$ – |
$ – |
|
| Miscellaneous |
$ – |
$ – |
$ – |
|
| Postage/Shipping |
$ – |
$ – |
$ – |
|
| Staff Travel |
$ – |
$ – |
$ – |
|
| Tele/Fax/E-mail |
$ – |
$ – |
$ – |
|
| Total Meeting Management |
$ – |
$– |
$ – |
|
| Total Expenses |
$ – |
$ – |
$ – |
|
| Net Income (loss) |
$ – |
$ – |
$ – |
|
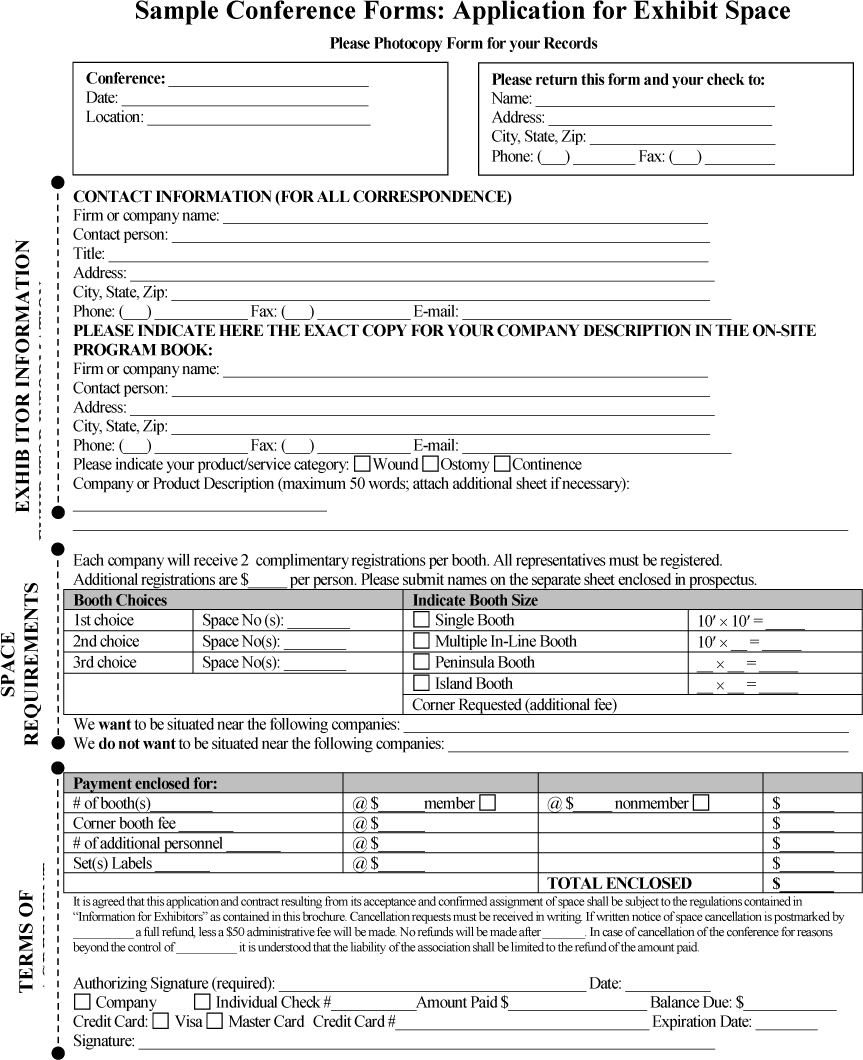
Sample Conference Forms: Exhibitor Evaluation Form
Conference or Seminar Name:
Date:
Location:
In order for _______________ to provide optimum arrangements for our exhibitors, we would appreciate your cooperation in completing this questionnaire. Please fill in the circle for rating of your choice.
| |
Excellent |
Good |
Fair |
Poor |
| 1. Please rate the interest level and quality of conference attendees in the exhibit hall. |
□ |
□ |
□ |
□ |
| 2. How would you rate overall attendance in the exhibit hall? |
□ |
□ |
□ |
□ |
| 3. How would you rate the effectiveness of the following exhibit days? |
| a. Date — Exhibits Open — time |
□ |
□ |
□ |
□ |
| b. Date — Exhibits Open — time |
□ |
□ |
□ |
□ |
| c. Date — Exhibits Open — time |
□ |
□ |
□ |
□ |
| d. Date — Exhibits Open — time |
□ |
□ |
□ |
□ |
| 4. How would you rate the adequacy of the exhibit hours? |
□ |
□ |
□ |
□ |
| 5. How would you rate the effectiveness of the exhibitor lead program? |
□ |
□ |
□ |
□ |
| 6. Please rate the quality of the following: |
| a. Exhibitor Registration Process |
□ |
□ |
□ |
□ |
| b. Hotel Accommodations |
□ |
□ |
□ |
□ |
| c. Exhibit Hall Design |
□ |
□ |
□ |
□ |
| d. Booth Location |
□ |
□ |
□ |
□ |
| e. Decorating |
□ |
□ |
□ |
□ |
| f. Cost of Booth |
□ |
□ |
□ |
□ |
| g. Overall Exposure to Attendees |
□ |
□ |
□ |
□ |
Sample Conference Forms: Conference Evaluation Form
Conference or Seminar Name:
Date:
Location:
To assist us in evaluating the effectiveness of this meeting and to make recommendations for the future, please complete this conference evaluation form by filling in the circle for the appropriate rating. Please complete the speaker portion of this form at the conclusion of each lecture. Return this form to the registration desk at the end of the conference along with the white copy of your certificate of attendance and contact hours form. Thank you for attending this meeting!
Section I. Overall Conference Evaluation
| |
Strongly Agree |
Agree |
Neutral |
Disagree |
Strongly Disagree |
| 1. I feel the conference achieved the following objectives: |
| a. (List objective) |
□ |
□ |
□ |
□ |
□ |
| b. (List objective) |
□ |
□ |
□ |
□ |
□ |
| 2. The conference met my personal objectives. |
□ |
□ |
□ |
□ |
□ |
| 3. The program was well organized. |
□ |
□ |
□ |
□ |
□ |
| 4. The exhibits provided an adequate environment for learning. |
□ |
□ |
□ |
□ |
□ |
| 5. The program book was easy to read and helpful. |
□ |
□ |
□ |
□ |
□ |
| 6. The individual sessions were relevant to the conference goals. |
□ |
□ |
□ |
□ |
□ |
| 7. The individual sessions assisted me in achieving my learning goals. |
□ |
□ |
□ |
□ |
□ |
Section II. Evaluation of Conference Quality
| |
Excellent |
Good |
Average |
Fair |
Poor |
| 1. Overall Conference |
□ |
□ |
□ |
□ |
□ |
| 2. Exhibits: |
| a. Grand Opening |
□ |
□ |
□ |
□ |
□ |
| b. Quality/Space |
□ |
□ |
□ |
□ |
□ |
| c. Time Allowed |
□ |
□ |
□ |
□ |
□ |
| d. Location |
□ |
□ |
□ |
□ |
□ |
| 3. Hotel Facilities |
□ |
□ |
□ |
□ |
□ |
| 4. Conference Registration |
□ |
□ |
□ |
□ |
□ |
| 5. Special Event |
□ |
□ |
□ |
□ |
□ |
| 6. Helpfulness of: |
| a. Planning Committee |
□ |
□ |
□ |
□ |
□ |
| b. Monitors/Moderators |
□ |
□ |
□ |
□ |
□ |
| c. Registration Personnel |
□ |
□ |
□ |
□ |
□ |
| d. Hotel Staff |
□ |
□ |
□ |
□ |
□ |
Section III. Content/Speaker Evaluation
| N/A = Not at All |
1 = Poor |
2 = Average |
3 = Above Average |
4 = Outstanding |
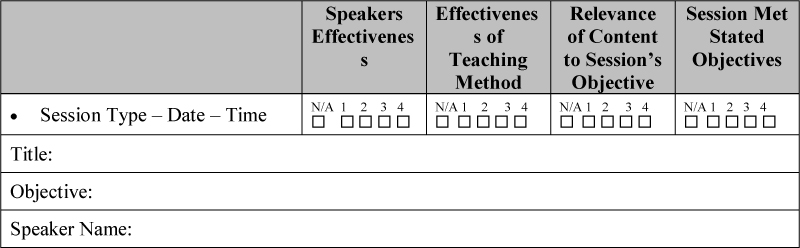
Appendix R: Role of the WOC Nurse or Continence Care Nurse in Continence Care
∗Note: This document was approved and adopted by the WOCN Society Board of Directors in 2009 and is available in the WOCN Public Library: http://www.wocn.org/PublicLibrary
Background
Incontinence (ie, loss of bladder and/or bowel control) is a significant health care problem, which affects an individual's physical and psychosocial life. The social costs of incontinence are high and even mild symptoms affect social, sexual, interpersonal, and professional function. Incontinence creates a burden on families and caregivers and has a significant economic impact on society.
The incidence of incontinence increases with age and is greatly impacted by factors that affect independent living. In 2000, the cost of incontinence was $12.6 billion. With increasing numbers of people who are 65 years of age and older, dealing with issues relating to incontinence will have a major economic impact on society.
Urinary Incontinence
Urinary incontinence is a stigmatized, underreported, underdiagnosed, and undertreated condition that is erroneously thought by many to be a normal part of aging.
- Nocturnal enuresis is the predominant type of incontinence among children.
- The incidence of incontinence among elderly nursing home residents is estimated to be 47% to 70% and is the second leading cause noted by caregivers for seeking nursing home placement.
- Fifty-three percent of homebound, older persons are incontinent or have overactive bladder/urge incontinence.
- One-third of men and women, 30 to 70 years of age, experience loss of bladder or bowel control at some point in their adult lives, one-third get out of bed 2 or more times per night to urinate, 1 in 8 reports losing urine in route to the bathroom, and two-thirds have never discussed bladder health with their doctor.
- Only 1 in 8 Americans who has experienced loss of bladder control has been diagnosed.
- On average, women wait 6.5 years from the first time they experience symptoms until they obtain a diagnosis for their bladder control problem(s).
- Men are less likely to be diagnosed than women.
- Men are also less likely to discuss incontinence with friends and family and are more likely to be uninformed.
- Two-thirds of individuals who experience loss of bladder control symptoms do not use any treatments or products to manage their incontinence.
- In the elderly population, the need for frequent toileting and/or urgency to void increases the risk of falls by 26% and bone fractures by 34%.
- It is estimated that approximately 80% of persons affected by urinary incontinence can be cured or improved.
- A recent study has shown that pelvic floor muscle training and bladder training resolved urinary incontinence in women as effectively as some anticholinergic drugs and were more effective than other approaches.
Fecal Incontinence
Fecal incontinence is the inability to control the passage of gas and/or liquid or solid stool.
- More than 5.5 million Americans are estimated to experience episodes of fecal incontinence.
- Six percent to ten percent of men and 6% to 15% of women experience fecal incontinence without urinary incontinence.
- More than 2% of all women (2.2%) who have delivered 1 or more children may experience fecal incontinence.
- Seven percent of healthy people, 65 years and older, experience fecal incontinence.
- Twenty-three percent of stroke patients experience fecal incontinence.
- Thirty-three percent of elderly people at home or in a hospital experience bowel control problems.
Combined Urinary and Fecal Incontinence (Dual Incontinence)
Dual incontinence impacts 25% of all US adults during their lives.
Role of the Continence Nurse
The continence nurse provides expert care to patients with urinary and/or fecal incontinence by conducting a focused assessment, performing a limited physical examination, synthesizing data, developing a plan of care, and evaluating interventions. The role includes, but is not limited to, serving as an expert clinician, consultant, educator, and/or administrator/manager in various health care settings.
Continence nursing management is based on an in-depth knowledge of normal voiding and defecation physiology, common alterations in bowel/bladder function and their sequelae, and a basic understanding of common diagnostic studies (eg, urinary analysis, culture and sensitivity, studies of the urinary and lower digestive tract).
Continence Nurse Competencies
Specific competencies of the continence nurse include the following skills and abilities:
- Performs a focused assessment.
- Obtains a relevant history.
- Performs bedside testing of bladder filling and sensation (bedside cystometrogram).
- Measures postvoid residual urine by catheterization or bladder scan.
- Synthesizes data related to incontinence to identify individuals at risk, reversible causes, types of urinary incontinence, and common bowel dysfunctions that contribute to fecal and/or urinary incontinence.
- Makes an appropriate nursing diagnosis of urge, stress, mixed, and/or functional urinary incontinence.
- Uses/recommends appropriate management strategies including the following interventions:
- Educates and counsels patients, families, and staff regarding:
- Behavioral therapies such as toileting programs, urge suppression, and pelvic muscle exercises.
- Bowel training or stimulated defecation programs.
- Intermittent self-catheterization.
- Care of indwelling urethral and suprapubic catheters.
- Incontinence products.
- Measures to clean, protect, and moisturize the perineal skin.
- Treatments for incontinence-related skin breakdown.
- Fluid and dietary modifications.
- Monitors therapeutic effects of medication therapy.
- Provides pelvic floor rehabilitation and reeducation via electrical muscle stimulation and biofeedback, in some settings.
- Evaluates outcomes of interventions and reports to the primary care provider as appropriate.
- Makes appropriate referrals for recurrent urinary tract infections, hematuria, pelvic organ prolapse, urinary retention, and pelvic pain syndromes.
- Monitors overall quality of care to identify needs for improvement.
Role of the Advanced Practice Continence Nurse
The advanced practice continence nurse provides expert care to patients with urinary and/or fecal incontinence by conducting a focused assessment, performing a comprehensive physical examination, synthesizing data, developing a plan of care, and evaluating interventions. The role includes, but is not limited to, serving as an expert clinician, consultant, educator, and/or administrator/manager in various health care settings.
Advanced Practice Nurse Continence Competencies
The advanced practice continence nurse possesses the competencies of the continence nurse and in addition has the following advanced competencies in accordance with an advanced level of education at the master's level and in accordance with state practice regulations:
- Performs a comprehensive physical assessment that may include a pelvic examination for masses, prolapse, and urethral hypermobility; a digital rectal examination of the prostate; and a neurologic assessment.
- Synthesizes data.
- Uses/recommends appropriate management strategies including the following interventions:
- Interprets diagnostic studies such as urodynamic studies and studies of bowel motility and elimination.
- Prescribes pharmacologic treatment of common conditions of the urinary tract and bowel such as urinary tract infection, overactive bladder, constipation, and diarrhea.
- Provides care for common gynecological conditions such as vaginitis and pelvic organ prolapse (ie, fitting and management of pessaries).
- Performs complex, multichannel urodynamic studies with/or without fluoroscopic imaging.
- Performs anorectal manometry studies.
- Provides pelvic floor rehabilitation and reeducation via electrical muscle stimulation and biofeedback.
Conclusion
The continence nurse is in an excellent position to meet the needs of patients with urinary and/or fecal incontinence across all practice settings. The continence nurse is skilled in the collaborative practice approach required for comprehensive patient management in today's health care environment.
Authors:
2008–2009 WOCN Continence Committee
2008–2009 WOCN Professional Practice Committee
Phyllis Kupsick, MSN, CS-FNP, CWOCN
Kate Lawrence, MSN, RN, CWOCN
Barbara Sadler, BSN, RN, CWOCN
Adopted by the WOCN Board of Directors: May 6, 2009
References
Bell, M., & DeMarinis, M. (2006). The psychological cost of incontinence. ECPN, 109, 13–14.
Bennett, H. (2005). Waking up dry: A guide to help children overcome bedwetting. Elk Grove Village, IL: American Academy of Pediatrics.
Bharucha, A., Zinsmeister, A., Locke, G., Seide, B., McKeon, K., Schleck, C., et al. (2005). Prevalence and burden of fecal incontinence: A population-based study in women. Gastroenterology, 129, 42–49.
Farrell, S. (2006). Cesarean section versus forceps-assisted vaginal birth: It's time to include pelvic injury in the risk-benefit equation. Canadian Medical Association Journal, 166, 337–338.
Hu, T., Wagner, T., Bentkover, J., Leblanc, K., Zhou, S., & Hunt, T. (2004). Costs of urinary incontinence and overactive bladder in the United States: A comparative study. Urology, 63, 461–465.
Landefeld, C., Bowers, B., Feld, A., Hartmann, K., Hoffman, E., Inglber, M., et al. (2008). National Institutes of Health state of the science statement: Prevention of fecal and urinary incontinence in adults. Annals of Internal Medicine, 148, 449–458. Retrieved May 5, 2008, from http://www.annals.org/cgi/content/full/0000605-200803180-00210v1
Lenderking, W., Nackley, J., Anderson, R., & Testa, M. (1998). A review of the quality of life aspects of urinary urge incontinence; Importance of patients' perspective and explanatory lifestyle. Journal of the American Geriatrics Society, 46, 683–692.
Martin, C. (1997). Urinary incontinence in the elderly. Consultant Pharmacist, 12. Retrieved from http://www.ascp.com/publications/tcp/1997/aug/elderly.html
Muller, N. (2005). What Americans understand and how they are affected by bladder control problems: Highlights of recent nationwide consumer research. Urologic Nursing, 25, 109–115.
National Association for Continence. (2008). What is incontinence? Retrieved May 5, 2008, from http://www.nafc.org/bladder-bowel-health
Palmeri, B., Giorgia, B., & Bellini, N. (2005). The anal bag: A modern approach to fecal incontinence management. Ostomy Wound Management, 51, 44–52.
Resnick, N. (1998). Improving treatment of urinary incontinence (commentary letter). Journal of the American Medical Association, 280, 2034–2035.
Saffel, D. (2006). Medication in the treatment of urinary incontinence. ECPN, 109, 27–31.
Shamliyan, T., Kane, R., Wyman, J., & Wilt, T. (2008). Systematic review: Randomized, controlled trials of nonsurgical treatments for urinary incontinence in women. Annals of Internal Medicine, 148, 459–473.
U.S. Department of Health and Human Services. (2007). Fecal incontinence. NIH Pub. 07–4866. Retrieved April 26, 2009, from http://digestive.niddk.nih.gov/ddiseases/pubs/fecalincontinence/fecalincontinence.pdf
Von Gontard, A., Schaumburg, H., Hollmann, E., Eiberg, E, & Rittig, S. (2001). The genetics of enuresis: A review. Journal of Urology, 166, 2438–2443.
Appendix S: WOCN Business Plan Template Workbook
Table of Contents
Acknowledgments
Developing a Business Plan
Appendix S–I. Sample Business Plan Template With Data
Appendix S–II. Sample Business Plan for Always Wright Consulting Services
Appendix S–III: A Business Financial Glossary
Acknowledgments
Contributors to the WOCN Business Plan Template Workbook
Wound, Ostomy and Continence Nurses Society
This document was developed by the WOCN Professional Practice Committee.
Business Plan Template Workbook Task Force:
Bianca Jones
Wound Care Nurse Consultant
UHS-Pruitt Corp
Norcross, GA
Sonya Perry, MSN, RN, CWOCN
Charleston Area Medical Center
Charleston, WV
Myra Varnado, BS, RN, CDE, CWOCN
LSU Hospital System
New Orleans, LA
Date Submitted: January 10, 2011
Resubmitted: April 18, 2011
Revised: May 2, 2011
Board Approval: July 26, 2011
Copyright© 2011 by the Wound, Ostomy and Continence Nurses Society. Date of Publication, August 2011.
No part of this publication may be reproduced, photocopied, or republished in any form, in whole or in part, without written permission of the Wound, Ostomy and Continence Nurses Society.
Developing a Business Plan
In this section, you will find a business plan template workbook designed to identify the specific components of a business plan and guide you through creating one for an existing or new business/product. As a wound, ostomy and continence (WOC) clinician, managerial leader, consultant, or advanced practice nurse, planning is an integral component of meeting organizational, departmental, and professional practice goals.
The concepts within this template will benefit the WOC nurse across a variety of health care settings. As a WOC nurse clinical leader, you know the advantage you provide in managing resources cost-effectively and affecting improved outcomes related to wound, ostomy, and incontinence care (Wound, Ostomy and Continence Nurses Society [WOCN], 2010). Whether you are a novice or experienced WOC nurse, your expert assessment and individualized plan of care influence long-term clinical outcomes across care systems.
Completion of a professional business plan demonstrates commitment to your goals for implementing best practices, serves as an educational tool that highlights your focus on improved patient outcomes, and provides an instrument for the expression of professional values.
Each part of the business plan template provides brief theoretical background, using questions to help you gather the information that will create a meaningful plan for your business model. You may find that not all content areas will apply to every business plan depending upon your business model as a sole proprietor or in a partnership.
Included in the business plan template are as follows:
- Introduction
- The Cover
- Present Situation
- Goals and Objectives
- Business/Product Description
- Market Analysis/Strategy
- Critical Success Factors/Key Assumptions
- Qualifications
- Budget Process
- Sample Contract
A sample business plan with data follows the workbook template. The information contained in the sample is fictitious and should not be considered valid to your plan. (See Appendix S–I: Sample Business Plan Template With Data.)
The business plan table of contents includes:
- Executive Summary
- Present Situation
- Goals and Objectives
- Business/Product Description
- Marketing Analysis and Strategy
- Critical Success Factors/Key Assumptions
- Staffing Structure
- Proposed Budget
- Appendices
The real value of creating a business plan lies in the process of researching and thinking about your goals in a systematic manner, more so than the finished product in hand. The act of planning helps you think through concepts thoroughly, study and research uncertain facts, and look at ideas critically. This takes time on the front end but often avoids costly mistakes later. The entire business plan template may take days and sometimes weeks to complete. Each question should be given serious thought and outside resources should be reviewed before completing most questions. After all the questions are answered, the actual business plan can be written. A formal written business plan will provide the greatest benefit to your process.
Planning a new business/product can be both exciting and intimidating. This business plan template will make the planning process easier. Adequate planning is the foundation of a successful business/product.
Introduction
- “He who fails to plan, plans to fail.” Proverb
“Success in business is threatened if you can't see the forest for the trees.” Unknown “In the absence of clearly defined goals, we are forced to concentrate on activity and ultimately become enslaved by it.”—Chuck Conradt (Marquis & Huston, 2006)
- What business endeavor, product, project, or proposal is you creating a business plan for (ie, private practice consultation, a small consulting business, continence or stoma clinics, skin care team, disease management program, etc)?
___________________________________________________________________________________________
___________________________________________________________________________________________
- Is this a new or existing business/product or clinical service?
_____________________________________________________________________________________
_____________________________________________________________________________________________
- Have you started the business plan? Yes□ No□
- Planning requires time: It typically takes several weeks to complete a good business plan. Most of that time will be utilized in research and rethinking/reworking your ideas and assumptions. Make time to complete the task thoroughly.
Be realistic and do not underestimate the time you will need to create a thorough and meaningful business plan or proposal. Whether you strive to improve clinical processes or you are requesting another WOC position to better meet current patient needs, planning will influence accomplishment. After the initial business plan is implemented, revising should be an ongoing process. You should collect information in your day-to-day activities and update the business plan 2 to 3 times a year. Minimally, you should revise your business plan with new goals and strategies at least once a year.
- How much time do you have to devote to a business or professional plan?
___________________________________________________________________________________________
___________________________________________________________________________________________
- When is the business plan due for presentation?
___________________________________________________________________________________________
___________________________________________________________________________________________
- How will you ration your time? _____hours per week for _____ weeks/months.
- Why develop a business plan?
A business plan is essential because it allows you to:
- Lay out the master blueprint to show a logical progression of steps needed to reach the established goal. It is a powerful management tool that also helps you consider alternatives or possibly a better way of doing things.
- Communicate your business plan to your own team. This is important in order to keep everyone on the same track and to be able to measure progress.
- Communicate your business plan to others to gain their support. This may come in the form of resources, financing, reimbursement, “word of mouth” referrals, or just plain moral support.
- Who on your team needs to be included in the business plan?
___________________________________________________________________________________________
___________________________________________________________________________________________
- Who else needs to receive your business plan?
___________________________________________________________________________________________
___________________________________________________________________________________________
Example: For a personal business or consulting business plan with an agency, include team members such as business partners, attorney, accountant/banker, and technology/end user consultant. Other recipients of the business plan include your key physicians and/or clinical partners.
If you as the clinical expert are creating a wound care program or an outpatient stoma clinic from within an agency or facility, include administrators, managers, nurses, and WOC nursing peers as appropriate. Depending on the scope of your services or proposal, you may seek guidance from the human resource department, data analyst, or an expert in billing and reimbursement. The knowledge, advice, and support you gain by collaborating with other leaders and thoroughly planning are critical to the business/product's success.
- Keys to convincing others
When others are looking at your business plan, their decision to support it depends heavily on the following areas:
- Your understanding of the current environment and your vision of the future: Your team's expertise—it is essential to identify the key attributes unique to a WOC nurse: the focused application of nursing science and practice to the care of persons of all ages with wounds, stomas, fistulae, drains, tubes, pressure ulcers, and incontinence (WOCN, 2010). You or your team must demonstrate that you have a balance of expertise in planning, educating, organizing, review/control, and leadership skills to impact patient care across health care systems.
- Your business/product—culturally sensitive and age-appropriate care planning for patients across a variety of delivery systems is essential. Holistic care and guidance for psychosocial, sexual, and body image adaptation promotes optimal client outcomes. You should be able to describe how your business/product is different from others and how it will address current and future health care needs.
Example: You may provide consultation in a remote service area without a formally educated or certified WOC nurse.
Refer to http://www.wocn.org and http://www.wocncb.org for more information about the value of board-certified WOC nurses. There are many ways that our training and expertise can influence positive measurable outcomes.
- Your marketing plan—market research is vital to the success of your business/product. There are 2 types of market research: (1) primary (gathering your own data) and (2) secondary (published information). You should have a strategy in place to market your business/product that includes expected growth as a result of marketing strategies. Wound, ostomy and continence nursing is a dynamic specialty that has been influenced by societal and health care needs of communities.
- Your projected financial statements—you should be able to show that support of the business plan will result in an expected financial outcome. This will include forecasted positive financial growth for your business/product and/or cost-effective utilization of resources with improved patient outcomes.
- Before you start
- Ask yourself:
- How much money is available (now)?
___________________________________________________________________________________________
- Where will the money come from?
___________________________________________________________________________________________
- Whom can I depend on for financial support?
___________________________________________________________________________________________
___________________________________________________________________________________________
- Will I leave a primary salaried (hourly) position with benefits?
___________________________________________________________________________________________
___________________________________________________________________________________________
- If so, will I be able to sustain myself financially until my business/product begins to profit?
___________________________________________________________________________________________
___________________________________________________________________________________________
- What outcomes/returns do I expect?
___________________________________________________________________________________________
___________________________________________________________________________________________
- What expertise do my team and I have?
___________________________________________________________________________________________
___________________________________________________________________________________________
- Will I work out of a home, office, or separate dwelling?
___________________________________________________________________________________________
___________________________________________________________________________________________
- How many hours am I/are we willing to invest?
___________________________________________________________________________________________
- Name your business/product:
- Keep it simple and straightforward.
- Be descriptive, include specifics.
- Make it distinctive.
- What key words describe your business/product?
___________________________________________________________________________________________
___________________________________________________________________________________________
- What will you name your business/product?
___________________________________________________________________________________________
___________________________________________________________________________________________
- Select outside advisors (identify which of the advisor/consultant experts you will utilize and who they are):
□ Attorney or legal council:
___________________________________________________________________________________________
___________________________________________________________________________________________
□ Management consultant, manager, or administrator:
___________________________________________________________________________________________
___________________________________________________________________________________________
□ Marketing consultant:
___________________________________________________________________________________________
___________________________________________________________________________________________
□ Accountant, value analysis manager:
___________________________________________________________________________________________
___________________________________________________________________________________________
□ Insurance agent:
___________________________________________________________________________________________
___________________________________________________________________________________________
□ Banker, billing, or reimbursement experts:
___________________________________________________________________________________________
___________________________________________________________________________________________
□ Other consultants such as information services/technology (IS/T) for Web page design and privacy and safety compliance experts for sharing or storing electronic patient records:
___________________________________________________________________________________________
___________________________________________________________________________________________
- Determine your “Unique Service Advantage”:
This is “That single, unique advantage, benefit, or appeal that others don't offer or do as well as you.”
You should consider years of experience, special skills or talents, particular areas of expertise, education, and service areas that are unique.
- What is unique about your business/product?
___________________________________________________________________________________________
___________________________________________________________________________________________
- What benefit(s) will your business/product bring that does not exist now?
___________________________________________________________________________________________
___________________________________________________________________________________________
- What is unique about you or your team?
___________________________________________________________________________________________
___________________________________________________________________________________________
- Building your business plan
Your business plan should look professional but not glitzy. It should be bound with a cover, printed on quality paper, and be produced with a laser or letter quality printer.
- What paper will you use for your business plan?
___________________________________________________________________________________________
- What color will the cover and coordinated paper be for your business plan?
___________________________________________________________________________________________
- How will you bind your business plan?
___________________________________________________________________________________________
- Will you need a quick print shop?
___________________________________________________________________________________________
- Which one?
___________________________________________________________________________________________
- How many copies of your business plan will you need?
___________________________________________________________________________________________
Consistent color coordination with your business/product logo, business cards, and stationary provides a professional presentation. Create a theme. Establish a Web site (even if it is only 1 page). This will present a professional appearance for yourself/business/product. If you will be presenting your business plan to a prospective client, remember to bring several hard copies of your business plan and always have a copy for your review during your interview.
The Cover
When you design the cover page of your business plan, keep the following in mind:
- Keep it simple.
- Clearly identify the business/product.
- Include address and phone numbers.
- Always date it.
- Indicate a contact person.
- What information do you want on your cover sheet?
- Name of business/product:
___________________________________________________________________________________________
- Address:
___________________________________________________________________________________________
- Phone number:
___________________________________________________________________________________________
- Date:
___________________________________________________________________________________________
- Contact person:
___________________________________________________________________________________________
- Contact person's credentials:
___________________________________________________________________________________________
- Contact person's qualifications:
___________________________________________________________________________________________
Table of Contents
A table of contents is imperative to facilitate the reader finding critical information with ease. The following is an ordered list of the usual contents of a business plan.
- Executive Summary
- Present Situation
- Objectives
- Business/Product Description
- Market Analysis/Strategy
- Operational Plan
- Financial Projections
- Appendix
Executive Summary
An executive summary is a critical but frequently overlooked portion of a business plan. It must be designed to capture the intended reader's interest by summarizing the key points and highlights of the business plan. It is a crystallization of the entire business plan in a brief overview format. Due to the nature of the executive summary, it is always located at the beginning of the business plan; however, it is one of the last portions that you will write.
A few things to remember when writing the executive summary are as follows:
- Keep it brief—1 page, if possible.
- Hit the high points—do not get bogged down in details.
- Make it interesting—you may want to change the summary for each intended reader and concentrate on the areas of most interest to that reader. Example: If presenting to physical therapist, explain how WOC nurse and rehab work together as a team.
Begin with a brief description of your business/product, how you developed it, and what your mission/purpose is. Next, describe the business/product that you will provide and how it will benefit the customer and/or the reader. (These topics should be stated succinctly in a few paragraphs.) One reference guide could be the information from Wound, Ostomy and Continence Nursing Certification Board “Are your Nurses Board Certified?” Do not assume that everyone is knowledgeable about the specific expertise and professional/clinical benefits provided by the WOC nurse.
Next, write a paragraph or two describing the background information including the market analysis, customer characteristics, competitive analysis, critical success factors, and assumptions.
Then spend sufficient time explaining your goals and strategies for obtaining them. This will lead easily into a summary of the financial picture and projections.
Close the executive summary with a 1-paragraph conclusion that highlights the points that you want this particular reader to remember.
Present Situation
Explain what factors and information have brought you to the decision to start this business/product. How does your business plan support the facility's mission statement and organizational goals?
- What changes are occurring in the health care environment, which will actually/potentially affect your business/product?
___________________________________________________________________________________________
___________________________________________________________________________________________
- What future changes or factors will impact your business/product? Include both those types of factors that will have a negative or a positive impact.
___________________________________________________________________________________________
___________________________________________________________________________________________
- External analysis
The following factors are important when analyzing the external environment (remember to do your homework and research these areas below):
- Demographics of the anticipated target patient population.
- Technology requirements.
- Regulatory/political.
- Economic/reimbursement.
What does the average person in your market area demographically look like? (You can usually find this information in the census bureau report; local, state, and federal reports; and other documents located in your local library or online.)
- Average age?
___________________________________________________________________________________________
- Fastest growing age group?
___________________________________________________________________________________________
- Average income?
___________________________________________________________________________________________
- Facility pressure ulcer prevalence and incidence?
___________________________________________________________________________________________
- Nonhealing wounds or patients with diabetes, and so forth?
___________________________________________________________________________________________
- Colon or bladder cancer incidence?
___________________________________________________________________________________________
- Continence or stoma clinics?
___________________________________________________________________________________________
- What is the primary industry?
___________________________________________________________________________________________
- Top 5 causes of mortality?
- ___________________________________________________________________________________________
- ___________________________________________________________________________________________
- ___________________________________________________________________________________________
- ___________________________________________________________________________________________
- ___________________________________________________________________________________________
- Top 5 causes of morbidity?
- ___________________________________________________________________________________________
- ___________________________________________________________________________________________
- ___________________________________________________________________________________________
- ___________________________________________________________________________________________
- ___________________________________________________________________________________________
- Other important information?
___________________________________________________________________________________________
- Competitive analysis
There are many types of competitors. Some of the most difficult competitors are the least obvious. The following are the 3 most common types:
- Input or resource—competes for the same resources as you.
- Process—provides a business/product that is different than yours but has many of the same results (ie, physical therapist, case managers).
- Output—does the exact same thing as you do.
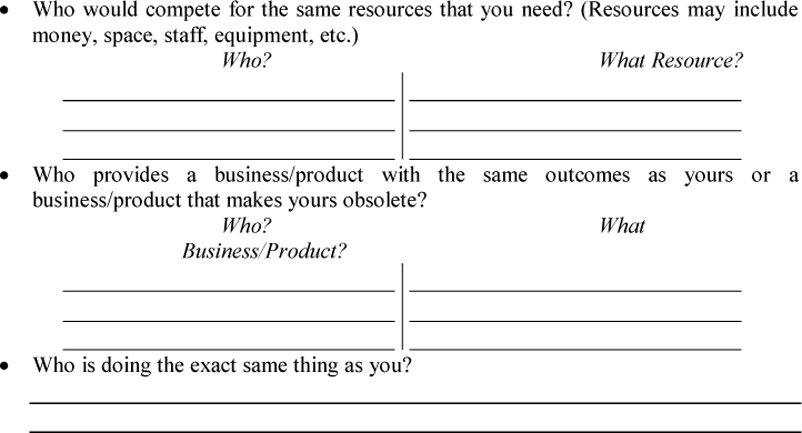
- Internal analysis
The following areas are the most common areas reviewed in an internal analysis.
- Past performance—can only be done when there is an existing business/product that has data from the past to analyze.
- Cost/profitability—reviews how profitable the business/product has been in the past. Profitability might be measured in actual revenue or net profit but could also be measured in other forms of benefits brought to an organization. Example: The business/product has been within budgeted expenses for the last 3 years and has had a net profit of “X” each year, or the business/product has stayed within the break-even projection and as a direct result of the business/product's activities, visits to the outpatient clinic have increased by 20%.
- Utilization—can be expressed in whatever units of measurement you prefer. It might be measured in any or all of the following: number of visits, hours, and patients. This is a representation of “volume” of service.
- Quality (customer perceived and technical)—technical quality is expressed as measurable outcomes and proven benefits. Perceived quality is from the customer's point of view. Sometimes what makes a customer satisfied is not necessarily technical quality. Example: Many patients have a high degree of satisfaction with a health care provider who is friendly and caring, even though his/her clinical skills may be less than adequate.
- Strengths and weaknesses—you must take a close look at what strengths and weaknesses you have. This can include an evaluation of your skills, your team's skills, financial strength, your support systems, your competitors, and any other factor that will impact your business/product.
- For EXISTING Businesses/Products Only:
How many “units” of service (ie, visits, hours, patients) compared to budget have you provided in the past 3 years?
- Unit of Service:
| Year 1: |
Actual:_____ |
Budget: |
| Year 2: |
Actual:_____ |
Budget: |
| Year 3: |
Actual:_____ |
Budget: |
- Unit of Service:
| Year 1: |
Actual:_____ |
Budget: |
| Year 2: |
Actual:_____ |
Budget: |
| Year 3: |
Actual:_____ |
Budget: |
- For All Existing and New Businesses/Products:
It is very important to capture this information on an ongoing basis.
- What proof do you have that your customers are satisfied or what types of methods will you use to measure your customers' satisfaction? (This information can include customer/patient satisfaction reports, written statements from patients, physicians, etc)
Goals and Objectives
Formulate a vision of where you want to be in 1 and 2 to 5 years and how you are going to get there. It is fine to be enthusiastic, but you should also be realistic. It is easiest to first set long-term goals and then establish a few objectives for each time period describing how you will achieve the goals. Do not get locked into a yearly time period; monthly time periods are very appropriate, especially for businesses/products.
Business/Product Description
Develop a clear explanation of what the business/product does and how it benefits your customers. To get support or financing for a business/product and to attract customers, you must show that you have researched and identified the need for the business/product. Moreover, you must be able to clearly describe the business/product and the benefits that it provides.
In a large organization, you cannot assume that others know what you do as a WOC specialty nurse. What is your vision? One of greatest contributions of leaders is having a driving purpose, a vision. This purpose is exhibited through your knowledge, passion, and experiences, and is reflective and empowers the group or culture (Grossman & Valiga, 2005).
The following are specific areas you need to consider:
- Service portfolio—WOC services, direct care, education, research, and standards.
- Unique features—these are specific to your business/product.
- Value-added benefits—program development expertise, disease management.
- Pricing strategy—this is unique to your situation and should reflect the economic environment, health care reform, and regulatory or market demands.
- What are the key features of your business/product?
___________________________________________________________________________________________
___________________________________________________________________________________________
- How do they differ from similar businesses/products?
___________________________________________________________________________________________
___________________________________________________________________________________________
- What value-added benefits does your business/product bring to your customers?
___________________________________________________________________________________________
___________________________________________________________________________________________
- Does your business/product save money for your customers? How?
___________________________________________________________________________________________
___________________________________________________________________________________________
- Does your business/product improve quality of life? How?
___________________________________________________________________________________________
___________________________________________________________________________________________
- Does your business/product create a competitive advantage? How?
___________________________________________________________________________________________
___________________________________________________________________________________________
- How do customers access your business/product?
___________________________________________________________________________________________
___________________________________________________________________________________________
- What are your hours of availability?
___________________________________________________________________________________________
___________________________________________________________________________________________
- Are you available for emergencies?
___________________________________________________________________________________________
___________________________________________________________________________________________
- What geographic area and care settings do you cover?
___________________________________________________________________________________________
___________________________________________________________________________________________
- How will the business/product evolve in the future?
___________________________________________________________________________________________
___________________________________________________________________________________________
Market Analysis and Strategy
Through market analysis, you can clearly identify your customers, your competitors, and your business/product's position in the market. This is the first and most important step in marketing. It is what will drive your marketing strategy and your promotional efforts. It helps you understand the needs of your customers, who your competition is, and where pitfalls lie. Give yourself adequate time to research and analyze this information. Market information can be obtained through analysis of past customer data, written or verbal surveys, and demographic information.
You can define your market in one way by the type of customer. The 3 types of customers are as follows:
- Decision maker—this is the customer who actually makes the decision to obtain your business/product. It may be the patient but also could easily be the physician or managed-care case manager, for example.
- Influencer—this customer influences the decision maker. It could be the patient's family, another nurse, and so forth.
- End user—this customer is the one who actually uses the business/product. The end user may also be the decision maker, but in health care the patient is frequently only the end user.
- Who are the consumers of your business/product?
- Who are the “decision makers?”
___________________________________________________________________________________________
___________________________________________________________________________________________
- Who are the “influencers?”
___________________________________________________________________________________________
___________________________________________________________________________________________
- Who are the “end users?”
___________________________________________________________________________________________
___________________________________________________________________________________________
- What characteristics and needs do your customers have?
- “Decision makers”
___________________________________________________________________________________________
___________________________________________________________________________________________
- “Influencers”
___________________________________________________________________________________________
___________________________________________________________________________________________
- “End users”
___________________________________________________________________________________________
___________________________________________________________________________________________
Once you have analyzed your market and your customers, you can begin to plan a marketing and promotional strategy. Based on the individual characteristics of each customer group, you can plan a strategy that will appeal to each. Keep in mind that one strategy does not usually apply to all 3 groups. Example: A case manager wants to hear how you will save money and achieve the expected outcomes. A patient, however, wants to know specifically what you will do and how available you are for phone calls.
When you plan your strategy, remember your Unique Service Advantage that you identified earlier. Focus strategies to highlight your uniqueness and benefits you bring to customers.
You will also need to decide what media you will use to market your business/product. If it is a business/product within an organization, a well-written, professional-looking business plan is the perfect medium. However, if it is an independent business/product, you will probably want to consider at least business cards, stationery, and perhaps brochures. Other techniques include the Internet, telephone books, human interest stories in the newspaper, speaking engagements, and face-to-face meetings. The key is to not get carried away and blow your budget on advertising and promotion. Start small, see what works, and then expand if you need to. Frequently, the most effective means of marketing a business/product is through word of mouth and networking. Go to where your customers are and talk to them!
- What key points do you want to convey to each customer group?
- “Decision makers”
___________________________________________________________________________________________
___________________________________________________________________________________________
- “Influencers”
___________________________________________________________________________________________
___________________________________________________________________________________________
- “End users”
___________________________________________________________________________________________
___________________________________________________________________________________________
- What media is best for each customer group?
- “Decision makers”
___________________________________________________________________________________________
___________________________________________________________________________________________
- “Influencers”
___________________________________________________________________________________________
___________________________________________________________________________________________
- “End users”
___________________________________________________________________________________________
___________________________________________________________________________________________
Critical Success Factors and Key Assumptions
Critical success factors are the conditions that must be met to achieve the success of your business/product. They may be resource related or situation related. Example: Your continence clinic will succeed only if there is adequate dedicated space available in the current outpatient setting, or your independent practice will succeed only if you obtain a contract with the local 400-bed hospital.
Assumptions are similar to critical success factors; however, they differ in that the success of the business/product is not dependent on them. Assumptions may also be resource or situation related. Frequently, assumptions are financial or utilization (volume of business—number of patients, hours, visits, etc) related. Example: Available space in the outpatient clinic becomes an assumption if there are several other space options available. Example: You assume that you will get a contract with the local 400-bed hospital and have based your financial analysis on that assumption. This is not a critical success factor if there are other contract options available.
- What resources are critical to the success of your business/product (ie, space, finances, personnel, equipment, etc)?
___________________________________________________________________________________________
___________________________________________________________________________________________
- What other factors are critical to the success of your business/product?
___________________________________________________________________________________________
___________________________________________________________________________________________
- What assumptions are you making as you plan your business/product?
___________________________________________________________________________________________
___________________________________________________________________________________________
Qualifications
The success of your business/product depends on the skills that you and your team possess. In addition, gaining support from others for your business/product will also depend on your ability to demonstrate that qualified individuals will be involved. Therefore, as you write your business plan, describe who will be in charge of the different aspects of the business/product and what other expertise you will use. Example: If you are the sole proprietor of an independent practice, you will want to describe your abilities, and the outside advisors that you have chosen (ie, attorney, accountant, etc).
For a business/product, it is likely that you will have several members of a team. The skills and responsibilities of each team member need to be clearly defined. Specific guidance documents or training classes may be necessary. It is helpful if several individuals are involved to identify specific responsibilities and explain who will manage each area. Example: Areas might be clinical services, reception, intake, billing, scheduling, marketing, quality improvement, purchasing, legal, accounting, and others as needed for your individual plan. Depending on how you are going to be using your business plan, you may want to include full resumes or curriculum vitae of individual team members in the Appendix of the plan.
You should also review the weaknesses of each team member. This is not a negative exercise. We all have areas in which we are less than perfect. Identifying those areas helps avoid putting people into situations in which they are sure to fail.
- Who are the members of your team? (Do not forget yourself!)
Financial Projections
It is critical in any business plan to formulate a pro forma budget that projects the expected revenues and expenses for 3 to 5 years or the length of the business/product and the break-even point. This helps you determine the validity of the business plan prior to starting the business/product and to evaluate progress over the ensuing years or life of the business/product.
Doing a pro forma is nothing more than creating an operating budget for the next 3 to 5 years. It should indicate at what point the business/product will break even and when it will start to show a profit. With businesses/products, the time frame may be in yearly quarters as opposed to entire years depending on the extent of the business/product.
- Financial fundamentals
There are several fundamental principles that you must understand in order to do a pro forma budget. You will most likely need to employ the services of an accountant to actually do the budget; however, you will still need to understand the concepts and be able to provide certain information to the accountant (See Appendix S–III: A Business Financial Glossary).
The first principle you need to understand is what a balance sheet and an income statement are used for and what information they contain.
- Balance sheet—a financial snapshot of a moment in time. A balance sheet profiles the overall financial condition of an organization. It can be likened to a complete physical assessment. It lets you know how things are at a given moment. The balance sheet specifically addresses a company's assets (or resources of value) and liabilities (or debts).
- Income statement—shows the results of operating activities. The income statement chronicles how a company got to the given moment in time that the balance sheet portrays. It can be likened to a record of how well or poorly a wound has healed over the past month. The income statement reports the total revenues (resources coming into the company), the expenses (resources going out of the company), and the net profit or net income (what's left over after expenses are paid). The income statement describes a period in time; it is usually done every month or every quarter.
A pro forma budget is nothing more than an income statement that projects the next 3 to 5 years.
It is not necessary to completely understand all the items on a balance sheet. Refer to an accountant for assistance. A sample balance sheet follows.
Balance Sheet as of April 30, 2011
| Assets |
Liabilities |
| Current assets |
Current liabilities |
| Property/plant/equipment |
Long-term debt |
| Investments |
Owners equity |
| Intangibles |
|
It is necessary to have some understanding of an income statement. However, it is not necessary to understand exactly how the numbers are calculated. Again, refer to an accountant for assistance. A sample of an income statement:
Income Statement for Period Ending April 30, 2011
| Revenue and Gains |
| Patient care revenues |
| Contract fees |
| |
| Operating Expenses |
| Salaries |
| Supplies |
| Administration |
| Depreciation |
| Utilities |
| Occupancy |
| |
| Net Income |
- Financial concepts
There are also several financial concepts that you must understand in order to compile the information that the accountant will need to put together your pro forma budget.
- Contractual allowances are like discounts. First, you will decide what your charge will be for a particular service. However, instances will occur in which you will need to discount your charge. This frequently happens with managed care contracts. If your charge is $80 but your managed care contract is for $75, the $5 difference is a contractual allowance. This amount will show up on the income statement in a format such as the following:
| Revenue: |
$80 |
| Less contractual allowance: |
$ (5) |
| Total revenue: |
$75 |
You must state your actual charge as revenue and then show your contractual allowances. You cannot just show the difference (ie, $75). This is an accounting rule that only accountants understand!
- Charity and bad debt are similar to contractual allowances except that they are not planned for as in a contract. Charity is a discount that you determine you will give prior to providing the service. Example: You can decide to give a 10% charity write-off to a patient who has limited financial resources. The amount the patient would actually pay of the $80 charge would be $72.
Bad debts are unplanned write-offs from what you had expected to receive for your services. Example: You billed a patient the $80 fee and he or she paid only $40 and never paid any more. After a period of time, you determine that this patient will never pay the remaining amount, and you write it off to bad debt.
Bad debt and charity write-offs are expressed on the income statement:
| Revenue (2 visits): |
$160 |
| Less charity of 10% for 1 visit: |
$ (8) |
| Less bad debt: |
$ (40) |
| Total revenue: |
$132 |
- Depreciation is the financial representation of the normal wear and tear on a large piece of equipment or property determined by taking the total value of the equipment or property and dividing it over a given number of years. This is also referred to as amortizing. The number of years is determined in many ways; the best thing to do is ask the accountant how many years to depreciate each piece of equipment you will need. Most organizations choose a specific dollar amount over which they will depreciate an item. Example: Anything over $500 or sometimes $1000 will be depreciated.
Example: You will need a biofeedback machine for your incontinence clinic that will cost $10,000. The accountant tells you that it will need to be depreciated over 5 years. The amount that will be “expensed” each year is $2000 ($10,000 divided by 5). The tricky part here is that the actual cash ($10,000) for the equipment will be spent when the equipment is purchased. However, the IRS will only let you recognize $2000 in expenses per year. In your pro forma budget, you will record an expense of $2000 each year for 5 years.
- When determining the costs that must be considered for your business/product, you will need to decide which are fixed and which are variable costs. Fixed costs are those costs that do not vary with the amount of services you provide. Example: Rent and depreciation on equipment are fixed. If your rent is $1000 per month, it does not matter whether you see 5 patients or 50 patients, the rent will not change. Variable costs are those costs that vary with the amount of services provided. Example: Patient care staff salaries and supplies will vary with the number of patients. You will use more supplies to see 50 patients than you will to see 5 patients.
- The importance of understanding fixed and variable costs is that you can control variable costs much more easily than you can control fixed costs. Frequently, you are more valuable to an organization as a variable cost than you are as a fixed cost. If you are a full-time employee with a set salary and benefits, you are a fixed cost. Whether you see 100 patients or 1000 patients, your salary and benefits will cost the organization the same. However, if you have a contract for a per unit fee, you are a variable cost. If your per unit fee is $75, the total amount the organization pays will vary with the number of units of service you provide. Therefore, if business is slow for your client (eg, a hospital), they can pay you for just the number of visits or amount of service that they need. When business is better, they are able to pay you for increased amounts of service.
The Budgeting Process
Now that you understand a few of the basic concepts, you are ready to begin collecting data for the pro forma budget. You must determine how much total revenue by source and total expenses by source you expect.
To determine the revenues and expenses, certain exercises are necessary:
- Statistical forecasting—trending
This is how you can determine the expected revenues for your business/product. If it is an existing business/product, you can use past data to forecast the coming year(s). If it is a new business/product, you will use your situation and market analyses to project the future years. This part of forecasting is based on utilization only. Example: You will determine the number of patients, procedures, visits, hours, and so forth, that you will provide. The unit to use is based on the mechanism by which you are paid. Example: If you are paid for the service by hour, you should project in hours, and so forth.
- Example:
| Patient Visits |
'10 |
'11 |
'12 |
% Forecast∗ |
'13 Projected |
| Ostomy |
500 |
460 |
440 |
3% |
426 |
| Wounds |
800 |
1000 |
1300 |
20% |
1560 |
| Continence |
300 |
550 |
700 |
30% |
910 |
| Total |
1600 |
2010 |
2440 |
19% |
2896 |
| ∗The forecast is calculated by averaging the % of increase for each of the past 3 years and then estimating any additional increase or decrease based on market factors. |
- Based on your analyses, complete the following chart:
| |
For Existing Businesses/Products |
For All Businesses/Products |
| Revenue Source |
Prior Year 1 |
Prior Year 2 |
Prior Year 3 |
Percent Forecast |
Projected Year 1 |
Projected Year 2 |
Projected Year 3 |
| |
|
|
|
|
|
|
|
| |
|
|
|
|
|
|
|
| |
|
|
|
|
|
|
|
| Total |
|
|
|
|
|
|
|
- Expense forecasting
Now, you will begin to think in dollar amounts. You will need to list all of your expenses and do the same type of trending that you did in the statistical forecasting.
Expenses that you should consider are as follows:
- Salaries/benefits—of all personnel (including yourself) involved in the business/product. You will need to know how much time will be worked and the salaries and benefits of each individual.
- Taxes and other employee expenses—the accountant can provide this information.
- Rent.
- Supplies/equipment—this includes only the supplies and equipment that will not be depreciated. You can also include your brochures, business cards, and office supplies here. Repairs on equipment can be included here also.
- Depreciation∗—this is where the $2000 of depreciation for the biofeedback machine in the example would be noted.
- Professional fees—this would include your outside advisors such as accountants, attorneys, and so forth.
- Dues/membership—you can include any professional journal subscriptions or memberships to professional organizations in this category.
- Education—this would include any seminars or conferences that you plan on attending. Expenses in this category include flight, mileage, food, lodging, and so forth, related to the educational event.
- Travel—these are travel costs associated with providing the service.
- Postage and shipping.
- Utilities—this would include phone, electric, gas, and so forth.
- Marketing/advertising—include any media that you will be using. This could be online marketing, telephone book listings, advertising, and other expenses associated with marketing. If you did not include your business cards and/or brochures under supplies, you could put them here.
- Miscellaneous—anything that cannot be reasonably classed in the aforementioned categories could be included here.
∗To determine your depreciation amount, you will need to list the “capital equipment” you need. Capital equipment is equipment that is over the depreciable limit set by you or the organization (usually $500 or $1000). Remember to ask the accountant about how many years the equipment needs to be depreciated.
- What depreciable equipment will you need?
| Equipment |
Cost |
Purchase Date |
Depreciable Years |
| Computer |
$2000 |
June |
5 |
| Printer |
$600 |
June |
5 |
| Copier |
$1000 |
June |
5 |
Again, if it is an existing business/product, you can use previous data to forecast; if it is a new business/product, you must use your best educated guess.
- Example:
| Expenses |
'10 |
'11 |
'12 |
% Forecast∗ |
'13 Projected |
| Salaries |
$50 |
$52.50 |
$80 |
38 |
110.40 |
| Rent |
$12 |
$12.60 |
$13.20 |
5 |
$13.80 |
| Other |
$20 |
$22 |
$25 |
0 |
$25 |
| Total |
$82 |
$87.10 |
$118.20 |
26 |
$149.40 |
| ∗The forecast is calculated by averaging the % of increase for each of the past 3 years and then estimating any additional increase or decrease based on market factors. |
- Complete the following chart to determine your projected expenses:
| |
For Existing Businesses/Products |
For All Businesses/Products |
| Expense Source |
Prior Year 1 |
Prior Year 2 |
Prior Year 3 |
% Forecast |
Projected Year 1 |
Projected Year 2 |
Projected Year 3 |
| |
|
|
|
|
|
|
|
| |
|
|
|
|
|
|
|
| |
|
|
|
|
|
|
|
| Total |
|
|
|
|
|
|
|
- Cost per unit
- The next step is to determine the average cost per unit based on your projections. It is calculated as follows:
- Average cost/unit = All expenses divided by the number of units
- Example: $149,400÷2896 = $52 per visit
- From your charts above, fill in the blanks to determine your projected average cost per unit for each year.
- Year 1:
Total expenses $_________÷Total number of units________ = $________per unit
- Year 2:
Total expenses $________÷Total number of units_____= $__________per unit
- Year 3:
Total expenses $________÷Total number of units _________ = $__________per unit
- Revenue forecast
Forecasting revenue is more difficult than forecasting expenses. There is no set rule for what your charge should be. Consideration must be given to what is charged for similar services, what the competition is charging, and what the market will bear. Wound, Ostomy and Continence Nurses Society compiled a salary and productivity survey of members in 2008. This beneficial tool can help you determine your fee for service based on your geographical location or expertise (WOCN, 2008).
| Setting |
Number of Respondents |
Median |
Average |
25th Percentile |
75th Percentile |
| Acute care |
28 |
$67.50 |
$73.82 |
$56.88 |
$81.25 |
| Home care |
34 |
$65 |
$66.91 |
$53.13 |
$80 |
| Subacute |
14 |
$65 |
$61.25 |
$50 |
$78.75 |
| Long-term care |
34 |
$65 |
$68.63 |
$50 |
$80 |
| Outpatient/wound care center |
13 |
$55 |
$63.40 |
$52 |
$65 |
| Education |
29 |
$77.50 |
$74.98 |
$50 |
$100 |
| Expert chart review |
22 |
$162.50 |
$164.80 |
$125 |
$200 |
| Depositions |
14 |
$250 |
$274.69 |
$200 |
$400 |
| Protocol development |
16 |
$77.50 |
$81.53 |
$45 |
$100 |
| Workshop |
20 |
$100 |
$129.47 |
$54.38 |
$150 |
If you have the luxury of using your charge in all cases, use the average cost per unit that you just calculated and add on an appropriate profit. If you have contracted rates that are different than your charge, you must consider the difference between your charge and the contracted rate. You will, however, most likely be charging different prices for different types of services.
- Example:
| Revenue Source |
Average Revenue/Unit |
Number of Visits |
Total $ |
| Ostomy |
$60 |
426 |
$25,560 |
| Wounds |
$72 |
1560 |
$112,320 |
| Continence |
$78 |
910 |
$70,980 |
| Total |
|
|
$208,860 |
- Determine your expected revenue by completing the following charts:
- Year 1:
| Revenue Source |
Revenue per Unit |
Number of Units |
Total Revenue |
| |
|
|
|
| |
|
|
|
| |
|
|
|
| Total |
|
|
|
- Year 2:
| Revenue Source |
Revenue per Unit |
Number of Units |
Total Revenue |
| |
|
|
|
| |
|
|
|
| |
|
|
|
| Total |
|
|
|
- Year 3:
/////////////////
| Revenue Source |
Revenue per Unit |
Number of Units |
Total Revenue |
| |
|
|
|
| |
|
|
|
| |
|
|
|
| Total |
|
|
|
- Break-even analysis
- The break-even analysis is important in determining how many units of service you need to provide in order to cover your expenses. It is calculated as follows:
- Average revenue/unit × Number of units = Total expenses
- Example: $70 × Number of units = $149,400
Number of units = $149,400 ÷ $70
Number of units = 2134
This means that 2134 visits are needed to cover expenses. It is not unusual for a new business/product to lose money the first year or so; however, you need to project when you expect to break even and then start making a profit. During the years that you will be breaking even or losing, you need to have financial support to at least pay your bills.
- Calculate your estimated break-even point:
- Year 1:
Average revenue/unit $_____ × Number of units _____ = Total expense $
Number of Units _____ = Total expense $_____ ÷ Average revenue/unit $
Number of units = _____
Breakeven? Yes □ No □
- Year 2:
Average revenue/unit $_____ × Number of units _____ = Total expense $
Number of units _____ = Total expense $_____ ÷ Average revenue/unit $
Number of units = _____
Breakeven? Yes □ No □
- Year 3:
Average revenue/unit $_____ × Number of units _____ = Total expense $
Number of units _____ = Total expense $_____ ÷ Average revenue/unit $
Number of units = _____
Breakeven? Yes □ No □
- Pro forma income statement
Believe it or not, this is the easiest part. Very simply put, the pro forma income statement indicates the revenue minus expenses—information you have already calculated. It finally shows you what your “bottom line” will be over the next 3 years.
Appendix
The Appendix of your business plan includes all the backup documents that support the data you have included in your business plan. Some of the documents you may want to include are as follows:
- External reports/information supporting your analyses.
- Charts and graphs from which you drew your projections.
- Product literature and lease agreements for capital requests.
- Marketing material you will use.
- Resumes of key members of the team.
Appendix S–I: Sample Business Plan for Always Wright Consulting Services
Introduction
- “He who fails to plan, plans to fail.” Proverb
“Success in business is threatened if you can't see the forest for the trees.” Unknown
“In the absence of clearly defined goals, we are forced to concentrate on activity and ultimately become enslaved by it.”—Chuck Conradt (Marquis & Huston, 2006)
- What business endeavor, product, project, or proposal is you creating a business plan for (ie, private practice consultation, a small consulting business, continence or stoma clinics, skin care team, disease management program, etc)? Private practice/consulting
- Is this a new or existing business/product or clinical service? New
- Have you started the business plan? Yes □ No ⊠
- Planning requires time: It typically takes several weeks to complete a good business plan. Most of that time will be utilized in research and rethinking/reworking your ideas and assumptions. Make time to complete the task thoroughly.
Be realistic and do not underestimate the time you will need to create a thorough and meaningful business plan or proposal. Whether you strive to improve clinical processes or you are requesting another wound, ostomy and continence (WOC) position to better meet current patient needs, planning will influence accomplishment. After the initial business plan is implemented, revising should be an ongoing process. You should collect information in your day-to-day activities and update the business plan 2 to 3 times a year. Minimally, you should revise your business plan with new goals and strategies at least once a year.
- How much time do you have to devote to a business plan? A few hours a week
- When is the business plan due for presentation? September 1, 2011
- How will you ration your time? 4 hours per week for 4 months.
- Why develop a business plan?
A business plan is essential because it allows you to:
- Lay out the master blueprint to show a logical progression of steps needed to reach the established goal. It is a powerful management tool that also helps you consider alternatives or possibly a better way of doing things.
- Communicate your business plan to your own team. This is important in order to keep everyone on the same track and to be able to measure progress.
- Communicate your business plan to others to gain their support. This may come in the form of resources, financing, reimbursement, “word of mouth” referrals, or just plain moral support.
- Who on your team needs to be included in the business plan?
Mary Smith—partner
Sally Jones—secretary/receptionist
Mark Williams—accountant
Sue Green—attorney
Richard Jones—small business consultant
- Who else needs to receive your business plan?
Gretchen Call—finance officer at First City Bank
Dr Steve Homes—supporter
Mike Miller—administrator, General Hospital
Example: For a personal business or consulting business plan with an agency, include team members such as business partners, attorney, accountant/banker, and technology/end user consultant. Other recipients of the business plan include your key physicians and/or clinical partners.
If you as the clinical expert are creating a wound care program or an outpatient stoma clinic from within an agency or facility, include administrators, managers, nurses, and WOC nursing peers as appropriate. Depending on the scope of your services or proposal, you may seek guidance from the human resource department, data analyst, or an expert in billing and reimbursement. The knowledge, advice, and support you gain by collaborating with other leaders and thoroughly planning are critical to the business/product's success.
- Keys to convincing others
When others are looking at your business plan, their decision to support it depends heavily on the following areas:
- Your understanding of the current environment and your vision of the future: Your team's expertise—it is essential to identify the key attributes unique to a WOC nurse: the focused application of nursing science and practice to the care of persons of all ages with wounds, stomas, fistulae, drains, tubes, pressure ulcers, and incontinence (Wound, Ostomy and Continence Nurses, 2010). You or your team must demonstrate that you have a balance of expertise in planning, educating, organizing, review/control, and leadership skills to impact patient care across health care systems.
- Your business/product—culturally sensitive and age-appropriate care planning for patients across a variety of delivery systems is essential. Holistic care and guidance for psychosocial, sexual, and body image adaptation promotes optimal client outcomes. You should be able to describe how your business/product is different from others and how it will address current and future health care needs.
Example: You may provide consultation in a remote service area without a formally educated or certified WOC nurse.
Refer to http://www.wocn.org and http://www.wocncb.org for more information about the value of board-certified WOC nurses. There are many ways that our training and expertise can influence positive measurable outcomes.
- Your marketing plan—market research is vital to the success of your business/product. There are 2 types of market research: (1) primary (gathering your own data) and (2) secondary (published information). You should have a strategy in place to market your business/product that includes expected growth as a result of marketing strategies. Wound, ostomy and continence nursing is a dynamic specialty that has been influenced by societal and health care needs of communities.
- Your projected financial statements—you should be able to show that support of the business plan will result in an expected financial outcome. This will include forecasted positive financial growth for your business/product and/or cost-effective utilization of resources with improved patient outcomes.
- Before you start
- Ask yourself:
- How much money is available (now)? Have $5000 seed money; will need a small business loan
- Where will the money come from? First City Bank and Small Business Administration
- Whom can I depend on for financial support?
Dr Steve Homes
Mike Miller
Dr Jessica Isle
Family
- Will I leave a primary salaried (hourly) position with benefits?
- If so, will I be able to sustain myself financially until my business/product begins to profit?
- Can you get support for the business/product? Yes
- What outcomes/returns do I expect? Enough business to equal or exceed my current income; a more autonomous work setting
- What expertise do my team and I have?
WOC clinical skills
Business development
Reimbursement
Inventory and supply control
- Will I work out of a home, office, or separate dwelling?
- How many hours am I/are we willing to invest? As much as it takes
- Name your business/product:
- Keep it simple and straightforward.
- Be descriptive, include specifics.
- Make it distinctive.
- What key words describe your business/product?
Consulting
Service oriented
Solutions to problems
- What will you name your business/product? Always Wright Consulting Services
- Select outside advisors (identify which of the advisor/consultant experts you will utilize and who they are):
⊠ Attorney or legal council: Sue Green
⊠ Management consultant, manager, or administrator: Richard Jones (SBA)
□ Marketing consultant:
⊠ Accountant, value analysis manager: Mark Williams
□ Insurance agent:
⊠ Banker, billing, or reimbursement experts: Gretchen Call
□ Other consultants such as information services/technology (IS/T) for Web page design and privacy and safety compliance experts for sharing or storing electronic patient records:
- Determine your “Unique Service Advantage”:
This is “That single, unique advantage, benefit, or appeal that others don't offer or do as well as you.”
You should consider years of experience, special skills or talents, particular areas of expertise, education, and service areas that are unique.
- What is unique about your business/product? Not only provides clinical WOC nursing as a variable cost but also combines an organizational development aspect to assist with program development
- What benefit(s) will your business/product bring that does not exist now? Combines the caring and service aspects of clinical care with a business perspective
- What is unique about you or your team? Extensive clinical experience with over 15 years in home care (the fastest growing health care setting), nurse with an MBA
- Building your business plan
Your business plan should look professional but not glitzy. It should be bound with a cover, printed on quality paper, and be produced with a laser or letter quality printer.
- What paper will you use for your business plan? My stationery, plain page
- What color will the cover and coordinated paper be for your business plan? Coordinated with my logo colors
- How will you bind your business plan? Velum binding
- Will you need a quick print shop? Yes
- Which one? Quik Print
- How many copies of your business plan will you need? 15
The Cover
When you design the cover page of your business plan, keep the following in mind:
- Keep it simple.
- Clearly identify the business/product.
- Include address and phone numbers.
- Always date it.
- Indicate a contact person.
- What information do you want on your cover sheet?
- Name of business/product: Always Wright Consulting Services
- Address: 1234 Maple Lane, Anywhere, PA 10023
- Phone number: (555) 123-4567
- Date: April 30, 2011
- Contact person: Kristy Wright
- Contact persons credentials: MBA, RN, CWOCN
- Contact persons qualifications: ______
Business Plan For:
Always Wright Consulting Services
April 30, 2011 |
Contact person:
Kristy Wright, MBA, RN, CWOCN
1234 Maple Lane
Anywhere, PA 10023
555-123-4567 |
Table of Contents
A table of contents is imperative to facilitate the reader finding critical information with ease. The following is an ordered list of the usual contents of a business plan.
- Executive Summary
- Present Situation
- Objectives
- Business/Product Description
- Market Analysis/Strategy
- Operational Plan
- Financial Projections
- Appendix
Executive Summary
An executive summary is a critical but frequently overlooked portion of a business plan. It must be designed to capture the intended reader's interest by summarizing the key points and highlights of the business plan. It is a crystallization of the entire business plan in a brief overview format. Due to the nature of the executive summary, it is always located at the beginning of the business plan; however, it is one of the last portions that you will write.
A few things to remember when writing the executive summary are as follows:
- Keep it brief—1 page, if possible.
- Hit the high points—do not get bogged down in details.
- Make it interesting—you may want to change the summary for each intended reader and concentrate on the areas of most interest to that reader. Example: If presenting to physical therapist, explain how WOCN and rehab work together as a team.
Begin with a brief description of your business/product, how you developed it, and what your mission/purpose is. Next, describe the business/product that you will provide and how it will benefit the customer and/or the reader. (These topics should be stated succinctly in a few paragraphs.) One reference guide could be the information for Wound, Ostomy and Continence Nursing Certification Board “Are your Nurses Board Certified?” Do not assume that everyone is knowledgeable about the specific expertise and professional/clinical benefits provided by the WOC nurse.
Next, write a paragraph or two describing the background information including the market analysis, customer characteristics, competitive analysis, critical success factors, and assumptions.
Then spend sufficient time explaining your goals and strategies for obtaining them. This will lead easily into a summary of the financial picture and projections.
Close the executive summary with a 1-paragraph conclusion that highlights the points that you want this particular reader to remember.
Present Situation
Explain what factors and information have brought you to the decision to start this business/product. How does your business plan support the facility's mission statement and organizational goals?
- What changes are occurring in the health care environment, which will actually/potentially affect your business/product? Managed care is increasing penetration in all health care settings in Western Pennsylvania. Many of the smaller hospitals and alternative settings are merging or affiliating to form larger networks. Everyone is trying to reduce costs and learn how to work more productively with managed care.
- What future changes or factors will impact your business/product? Include both those types of factors that will have a negative or a positive impact.
- External analysis
The following factors are important when analyzing the external environment (remember to do your homework and research these areas below):
- Demographics of the anticipated target patient population.
- Technology requirements.
- Regulatory/political.
- Economic/reimbursement.
What does the average person in your market area demographically look like? (You can usually find this information in the census bureau report; local, state, and federal reports; and other documents located in your local library or online.)
- Average age? 73 years old
- Fastest growing age group? Over 80
- Average income? $25,000
- Facility pressure ulcer prevalence and incidence?
- Nonhealing wounds or diabetes patients, and so forth?
- Colon or bladder cancer incidence?
- Continence or stoma clinics?
- What is the primary industry? Manufacturing
- Top 5 causes of mortality?
- Heart disease
- Diabetes (endocrine disorders)
- Traffic accidents
- Cancer
- Circulatory disorders
- Top 5 causes of morbidity?
- Heart disease (congestive heart failure)
- Diabetes
- Circulatory disorders
- Cancer (lung, breast, bladder)
- Mental illness
- Other important information? The most costly diseases and disorders are congestive heart failure, wounds, and chronic peripheral vascular disease. One city (population approximately 20,000) has a significantly higher occurrence of bladder cancer. Due to the elderly population throughout the region, there is a high and relatively untreated incidence of incontinence. The long-term care facilities view this as their greatest concern followed closely by pressure ulcers. A growing health care workers' shortage and the impending entrance of the baby boomers to the age group older than 65 years will put an additional strain on all systems.
- Competitive analysis
There are many types of competitors. Some of the most difficult competitors are the least obvious. The following are the 3 most common types:
- Input or resource—competes for the same resources as you.
- Process—provides a business/product that is different than yours but has many of the same results (ie, physical therapist, case managers).
- Output—does the exact same thing as you do.
- Who would compete for the same resources that you need? (Resources include money, space, staff, equipment, etc).
| Who? |
What Resource? |
| Not applicable |
Not applicable |
- Who provides a business/product with the same outcomes as yours or a business/product that makes yours obsolete?
| Who? |
What Business/Product? |
| Physical therapists |
Wound care |
| ABC Physician Group |
Wound care |
- Who is doing the exact same thing as you? Two other WOC nurses in the area
- Internal analysis
The following areas are the most common areas reviewed in an internal analysis.
- Past performance—can only be done when there is an existing business/product that has data from the past to analyze.
- Cost/profitability—reviews how profitable the business/product has been in the past. Profitability might be measured in actual revenue or net profit but could also be measured in other forms of benefits brought to an organization. Example: The business/product has been within budgeted expenses for the last 3 years and has had a net profit of “X” each year, or the business/product has stayed within the break-even projection and as a direct result of the business/product's activities, visits to the outpatient clinic have increased by 20%.
- Utilization—can be expressed in whatever units of measurement you prefer. It might be measured in any or all of the following: number of visits, hours, and patients. This is a representation of “volume” of service.
- Quality (customer perceived and technical)—technical quality is expressed as measurable outcomes and proven benefits. Perceived quality is from the customer's point of view. Sometimes what makes a customer satisfied is not necessarily technical quality. Example: Many patients have a high degree of satisfaction with a health care provider who is friendly and caring, even though his/her clinical skills may be less than adequate.
- Strengths and weaknesses—you must take a close look at what strengths and weaknesses you have. This can include an evaluation of your skills, your team's skills, financial strength, your support systems, your competitors, and any other factor that will impact your business/product.
- For EXISTING Businesses/Products Only: This is a new business, so this section does not apply
How many “units” of service (ie, visits, hours, patients) compared to budget have you provided in the past 3 years?
- Unit of Service: N/A
| Year 1: |
Actual: _____ |
Budget: _____ |
| Year 2: |
Actual: _____ |
Budget: _____ |
| Year 3: |
Actual: _____ |
Budget: _____ |
- Unit of Service: N/A
| Year 1: |
Actual: _____ |
Budget: _____ |
| Year 2: |
Actual: _____ |
Budget: _____ |
| Year 3: |
Actual: _____ |
Budget: _____ |
- For All Existing and New Businesses/Products:
It is very important to capture this information on an ongoing basis
- What proof do you have that your customers are satisfied or what types of methods will you use to measure your customers' satisfaction? (This information can include customer/patient satisfaction reports, written statements from patients, physicians, etc) Customer satisfaction will be measured through random phone interviews during the provision of services and mailed satisfaction surveys (with self-addressed stamped envelopes).
- What are your strengths and weaknesses?
- Technical skills:
| Strengths |
Weaknesses |
Ostomy and wound care
incontinence care
Home care
Reimbursement |
Diagnostic skills in Outcomes data |
- Business skills:
| Strengths |
Weaknesses |
Organizational development
Financial analysis
Marketing
Medical equipment/supplies |
Inability to negotiate capitated contract
“Sales” experience |
- Other skills/talents:
| Strengths |
Weaknesses |
Well known in community org.
Years of experience system
Certified in quality improvement |
Not well known by managed care
Not affiliated with a large |
- What are your team's strengths?
- Technical skills:
| Strengths |
Weaknesses |
Continence care
Complex clinical assessment
Burn therapy |
Complex ostomy care |
- Business skills:
| Strengths |
Weaknesses |
Billing and bookkeeping
Customer service |
Database management |
- Other skills/talents:
| Strengths |
Weaknesses |
Certified in critical care nursing
Certified in rehab nursing |
Public speaking |
- What financial strengths and weaknesses do you have?
| Strengths |
Weaknesses |
Seed money of $5000
Small business loan
Two guaranteed contracts |
Uncertain income |
- Who supports you? Who does not?
| Does |
Does not |
Dr Homes
Mike Miller—administrator
Dr Becket |
Peg Nando—previous boss
Hawk PT Group |
- What can you do better than your competitors? Provide a comprehensive service that not only includes clinical services but also offers protocol development, business development (ie, outpatient services), marketing to managed care, and assistance with reimbursement
- What can your competitors do better than you? Patients can get direct reimbursement, one WOC nurse has experience with capitated contracts, and the other WOC nurse has an established wound clinic
- What other things do you do well? Skilled at education and public presentation
Goals and Objectives
Formulate a vision of where you want to be in 1 and 2 to 5 years and how you are going to get there. It is fine to be enthusiastic, but you should also be realistic. It is easiest to first set long-term goals and then establish a few objectives for each time period describing how you will achieve the goals. Do not get locked into a yearly time period; monthly time periods are very appropriate, especially for businesses/products.
- What are your goals?
Here are a few things to consider in setting goals.
- When do you want to open or start the business/product? September 1, 2011
- Do you want to stay a sole proprietor? No
- Have partners? One now and then more
- When do you want to break even? 12 to 18 months
- Make a profit? 18 to 24 months
- What kind of financial growth do you want over the next 5 years? Modest with 10% to 15% each year
- How many patients/hours/units of service do you want to provide/serve over the next 5 years? Would like to increase contracts from the 2 current guaranteed contracts by obtaining contracts with at least 1 other hospital and include home- and long-term care. It seems realistic for each of the 2 WOC nurses in the practice to average 5 to 6 patients per day—equating to approximately 2600 patients per year. A modest 10% growth would result in approximately 3400 patients in 5 years. This would obviously require additional WOC nurses (at least part-time).
- What debts must you incur to start the business/product and when do you want to have your start-up costs paid off? (Normally it takes 2–3 years to pay off start-up costs for supplies and 5–10 years for equipment.) Initially, start-up costs will be small. We will need about $5000 for equipment and office supplies. Rent and utilities will average about $150 per month. The largest debt at first will be payroll until the first billing period. The small business loan should cover those expenses for 6 months. I would like the initial loans to be paid off in no later than 5 years.
- What do you need to do to overcome your identified weaknesses? Become more knowledgeable about capitated contracting, start collecting outcome data, and develop ties with health systems.
- What other things do you need to consider? Education of other team members, ways to grow the business.
- List at least 3 goals you want to achieve over the next 3 to 5 years:
- Achieve a 10% to 15% growth over each of the next 5 years
- Pay off start-up debt in 5 years
- Realize a profit in 2 years
- Assure quality of services with measured outcomes
- Employ qualified team members
- Fill out the following charts:
- Goal 1: Achieve a 10% to 15% growth over each of the next 5 years.
| Steps to Achieve |
Resources Needed |
Completion Date |
| Get contract with 2 hospitals |
None additional |
December 2012 |
| Get contract with 3 home care organizations |
Possibly half-time WOC nurse, funding, staffing, van, equipment |
March 2013 |
| Establish outpatient clinic |
Funding, staffing, space |
December 2015 |
| Establish mobile clinic |
Funding, staffing, van, equipment |
December 2016 |
- Goal 2: Pay off start-up debt in 5 years.
| Steps to Achieve |
Resources Needed |
Completion Date |
| Put 5% of revenue toward loans each quarter |
Adequate revenue |
Each quarter, ending in 2016 |
- Goal 3: Realize a profit in 2 years.
| Steps to Achieve |
Resources Needed |
Completion Date |
| Get contract with 2 hospitals |
None additional |
December 2012 |
| Get contract with 3 home care organizations |
Possibly half-time WOC nurse, funding, staffing, van, equipment |
March 2013 |
- Goal 4: Ensure quality of service with measured outcomes.
| Steps to Achieve |
Resources Needed |
Completion Date |
| Develop clinical guidelines for practice |
WOCN guidelines |
December 2012 |
| Set up database to collect outcome data |
Education for secretary on database management |
March 2013 |
| Analyze and report data |
Time!!! |
September 2013 |
- Goal 5: Employ qualified team members.
| Steps to Achieve |
Resources Needed |
Completion Date |
| WOC nurses to attend WOCN conferences |
Funding and patient coverage |
Annually |
| WOC nurses to be certified |
Funding |
Every 5 years |
| Database management education for secretary |
Funding and time |
March 2013 |
Business/Product Description
Develop a clear explanation of what the business/product does and how it benefits your customers. To get support or financing for a business/product and to attract customers, you must show that you have researched and identified the need for the business/product. Moreover, you must be able to clearly describe the business/product and the benefits that it provides.
In a large organization, you cannot assume that others know what you do as a WOC specialty nurse. What is your vision? One of greatest contributions of leaders is having a driving purpose, a vision. This purpose is exhibited through your knowledge, passion, and experiences, and is reflective and empowers the group or culture (Grossman & Valiga, 2005).
The following are specific areas you need to consider:
- Service portfolio—WOC services, direct care, education, research, and standards.
- Unique features—these are specific to your business/product.
- Value-added benefits—program development expertise, disease management.
- Pricing strategy—this is unique to your situation and should reflect the economic environment, health care reform, and regulatory or market demands.
- What are the key features of your business/product? Clinical services and consultation: prevention, patient education, and comprehensive management for patients with wounds, ostomies, and incontinence.
Case management: coordination, resource utilization, continuity, patient advocacy, and long-term management.
Education and development: protocol development, staff education, program development (ie, outpatient clinics, continuum of care), and regulatory compliance.
Research: clinical trials and outcome development.
- How do they differ from similar businesses/products? Other similar services concentrate on providing only the clinical piece. My service will provide a more comprehensive approach to the care of wound, ostomy and continence patients and will be available in all settings.
- What value-added benefits does your business/product bring to your customers? Contracting for services is a variable cost rather than a fixed cost. Assistance with resource management (ie, supplies) and reimbursement will ensure that services are revenue producing for the customer whenever possible. Assess and identify areas of opportunity related to pressure ulcer prevention, incontinence, or chronic wound management. Provide assistance with regulatory compliance through staff education, protocol development, and quality measurement. Decreased costs in a capitated system due to decreased length of stay, availability of services in the most appropriate setting, decreased complications, and decreased readmission to higher level of acuity.
- Does your business/product save money for your customers? How? Yes, resource management—care provided in most cost-effective setting, reduced complications, and risk management.
- Does your business/product improve quality of life? How? Yes, patient education, continuity, family involvement, decreased complications, and more rapid return to normal activities of daily living.
- Does your business/product create a competitive advantage? How? Yes, having the comprehensive services available in all settings as a variable cost puts the organization in a better position to negotiate with managed care organizations for capitated agreements.
- How do customers access your business/product? Phone: available 8 am to 5 pm Monday to Friday, with 24-hour on call and emergency service available through an answering service. “Quick Referral”—a referral form will be available that can be faxed 24 hours or e-mailed to [email protected].
- What are your hours of availability? 8 am to 5 pm, with 24-hour on call and emergency.
- Are you available for emergencies? Yes
- What geographic area and care settings do you cover? Butler, Armstrong and Lawrence Counties, and Alle-Kiski Valley. Acute, outpatient, home care, and long-term care settings.
Market Analysis and Strategy
Through market analysis, you can clearly identify your customers, your competitors, and your business/product's position in the market. This is the first and most important step in marketing. It is what will drive your marketing strategy and your promotional efforts. It helps you understand the needs of your customers, who your competition is, and where pitfalls lie. Give yourself adequate time to research and analyze this information. Market information can be obtained through analysis of past customer data, written or verbal surveys, and demographic information.
You can define your market in one way by the type of customer. The 3 types of customers are as follows:
- Decision maker—this is the customer who actually makes the decision to obtain your business/product. It may be the patient but also could easily be the physician or managed-care case manager, for example.
- Influencer—this customer influences the decision maker. It could be the patient's family, another nurse, and so forth.
- End user—this customer is the one who actually uses the business/product. The end user may also be the decision maker, but in health care the patient is frequently only the end user.
- Who are the consumers of your business/product?
- Who are the “decision makers?”
Physicians
Administrators
Case managers
Sometimes the patient/family
- Who are the “influencers?”
Staff nurses
Other clinical personnel in the care setting
Family
Some physicians
- Who are the “end users?”
Patients
Families/caregivers
Administrators for program development
- What characteristics and needs do your customers have?
- “Decision makers”
Physicians are interested in getting services for their patients with as few hassles for themselves as possible
Case managers are concerned with the least cost in the most appropriate setting and satisfied patients
Administrators want cost reduction, compliance with regulation, and satisfied customers
- “Influencers”
They are usually other health care professionals
They are concerned primarily about the quality of the services and care of the patient
When it is family, they are usually the caregiver or are responsible for the patient's care
- “End users”
Patients and families want timely, consistent, high-quality care
They want to be at home if possible
Once you have analyzed your market and your customers, you can begin to plan a marketing and promotional strategy. Based on the individual characteristics of each customer group, you can plan a strategy that will appeal to each. Keep in mind that 1 strategy does not usually apply to all 3 groups. Example: A case manager wants to hear how you will save money and achieve the expected outcomes. A patient, however, wants to know specifically what you will do and how available you are for phone calls.
When you plan your strategy, remember your Unique Service Advantage that you identified earlier. Focus strategies to highlight your uniqueness and benefits you bring to customers.
You will also need to decide what media you will use to market your business/product. If it is a business/product within an organization, a well-written, professional-looking business plan is the perfect medium. However, if it is an independent business/product, you will probably want to consider at least business cards, stationery, and perhaps brochures. Other techniques include the Internet, telephone books, human interest stories in the newspaper, speaking engagements, and face-to-face meetings. The key is to not get carried away and blow your budget on advertising and promotion. Start small, see what works, and then expand if you need to. Frequently, the most effective means of marketing a business/product is through word of mouth and networking. Go to where your customers are and talk to them!
- What key points do you want to convey to each customer group?
- “Decision makers”
“Quick Referral” service available
Use of services decreases short- and long-term costs
Patients can return to less acute settings and still receive services
“Comprehensive” services are available in addition to clinical services
- “Influencers”
Services will result in faster recovery, higher quality of life, and are easily accessible
- “End users”
Services are available 24 hours and are easily accessible
Staff are competent and experienced professionals
Services will allow patient to be at home if at all possible
- What media is best for each customer group?
- “Decision makers”
Brochure (designed for the professional; emphasizing the benefits and value added)
Follow-up (either verbal or in writing) whenever appropriate
Face-to-face visits
Networking
- “Influencers”
Staff in-services word of mouth “working together” on cases
- “End users”
Article in paper
Community involvement
Patient/customer-oriented brochure
Critical Success Factors and Key Assumptions
Critical success factors are the conditions that must be met to achieve the success of your business/product. They may be resource related or situation related. Example: Your continence clinic will succeed only if there is adequate dedicated space available in the current outpatient setting, or your independent practice will succeed only if you obtain a contract with the local 400-bed hospital.
Assumptions are similar to critical success factors; however, they differ in that the success of the business/product is not dependent on them. Assumptions may also be resource or situation related. Frequently, assumptions are financial or utilization (volume of business—number of patients, hours, visits, etc) related. Example: Available space in the outpatient clinic becomes an assumption if there are several other space options available. Example: You assume that you will get a contract with the local 400-bed hospital and have based your financial analysis on that assumption. This is not a critical success factor if there are other contract options available.
- What resources are critical to the success of your business/product (ie, space, finances, personnel, equipment, etc)?
Office space
Phone/fax
Computer and printer
E-mail service
Copy machine
Capital to underwrite business for 6 months
Personnel: Two WOC nurses and a secretary
- What other factors are critical to the success of your business/product? We need at least the 2 hospital contracts.
- What assumptions are you making as you plan your business/product? That 2 of the 5 home care organizations will affiliate with the 2 contracted hospital. One of the WOC nurses now working in a hospital will be willing to come into the practice in 12 to 18 months
Qualifications
The success of your business/product depends on the skills that you and your team possess. In addition, gaining support from others for your business/product will also depend on your ability to demonstrate that qualified individuals will be involved. Therefore, as you write your business plan, describe who will be in charge of the different aspects of the business/product and what other expertise you will use. Example: If you are the sole proprietor of an independent practice, you will want to describe your abilities, and the outside advisors that you have chosen (ie, attorney, accountant, etc).
For a business/product, it is likely that you will have several members of a team. The skills and responsibilities of each team member need to be clearly defined. Specific guidance documents or training classes may be necessary. It is helpful if several individuals are involved to identify specific responsibilities and explain who will manage each area. Example: Areas might be clinical services, reception, intake, billing, scheduling, marketing, quality improvement, purchasing, legal, accounting, and others as needed for your individual plan. Depending on how you are going to be using your business plan, you may want to include full resumes or curriculum vitae of individual team members in the Appendix of the plan.
You should also review the weaknesses of each team member. This is not a negative exercise. We all have areas in which we are less than perfect. Identifying those areas helps avoid putting people into situations in which they are sure to fail.
- Who are the members of your team? (Do not forget yourself!)
Kristy Wright
Mary Smith—partner
Sally Jones—secretary/receptionist
Mark Williams—accountant
Sue Green—attorney
Richard Jones—small business consultant
- What are the strengths and weakness of each?
- Member: Kristy Wright, MBA, RN, CWOCN
| Strengths |
Weaknesses |
Twenty years of WOC experience
Fifteen years in administration
Organized/efficient
“Big-picture” |
Lack of clinical incontinence experience
Lack of experience with capitation |
- Member: Mary Smith, MSN, RN, CWOCN
| Strengths |
Weaknesses |
Certified critical care
Certified rehabilitation
Excellent clinical skills |
Little experience w/ostomy care
No “business” experience |
- Member: Sally Jones, Secretary/Receptionist
| Strengths |
Weaknesses |
Medical secretary
Medical transcriptionist
Experience in customer service |
Limited database management
Financial record keeping |
- Who will be responsible for each functional area?
- Area: Practice management
Kristy Wright
- Area: Clinical services
Kristy Wright
Mary Smith
- Area: Organizational development service
Kristy Wright
Mary Smith
Sally Jones
- Area: Marketing
Kristy Wright
Sally Jones
Richard Jones
- Area: Bookkeeping/accounting
Mark Williams
Sally Jones
- Area: Legal
Sue Green
Financial Projections
It is critical in any business plan to formulate a pro forma budget that projects the expected revenues and expenses for 3 to 5 years or the length of the business/product and the break-even point. This helps you determine the validity of the business plan prior to starting the business/product and to evaluate progress over the ensuing years or life of the business/product.
Doing a pro forma is nothing more than creating an operating budget for the next 3 to 5 years. It should indicate at what point the business/product will break even and when it will start to show a profit. With businesses/products, the time frame may be in yearly quarters as opposed to entire years depending on the extent of the business/product.
- Financial fundamentals
There are several fundamental principles that you must understand in order to do a pro forma budget. You will most likely need to employ the services of an accountant to actually do the budget; however, you will still need to understand the concepts and be able to provide certain information to the accountant (See Appendix S–III. A Business Financial Glossary).
The first principle you need to understand is what a balance sheet and an income statement are used for and what information they contain.
- Balance sheet—a financial snapshot of a moment in time. A balance sheet profiles the overall financial condition of an organization. It can be likened to a complete physical assessment. It lets you know how things are at a given moment. The balance sheet specifically addresses a company's assets (or resources of value) and liabilities (or debts).
- Income statement—shows the results of operating activities. The income statement chronicles how a company got to the given moment in time that the balance sheet portrays. It can be likened to a record of how well or poorly a wound has healed over the past month. The income statement reports the total revenues (resources coming into the company), the expenses (resources going out of the company), and the net profit or net income (what's left over after expenses are paid). The income statement describes a period in time; it is usually done every month or every quarter.
A pro forma budget is nothing more than an income statement that projects the next 3 to 5 years.
It is not necessary to completely understand all the items on a balance sheet. Refer to an accountant for assistance. A sample balance sheet follows.
| Balance Sheet as of April 30, 2011 |
| Assets |
Liabilities |
| Current assets |
Current liabilities |
| Property/plant/equipment |
Long-term debt |
| Investments |
Owners equity |
| Intangibles |
|
It is necessary to have some understanding of an income statement. However, it is not necessary to understand exactly how the numbers are calculated. Again, refer to an accountant for assistance. A sample of an income statement:
| Income Statement for Period Ending April 30, 2011 |
Revenue and Gains
Patient care revenues
Contract fees |
Operating Expenses
Salaries
Supplies
Administration
Depreciation
Utilities
Occupancy |
| Net Income |
- Financial concepts
There are also several financial concepts that you must understand in order to compile the information that the accountant will need to put together your pro forma budget.
- Contractual allowances are like discounts. First, you will decide what your charge will be for a particular service. However, instances will occur in which you will need to discount your charge. This frequently happens with managed care contracts. If your charge is $80 but your managed care contract is for $75, the $5 difference is a contractual allowance. This amount will show up on the income statement in a format such as the following:
| Revenue: |
$80 |
| Less contractual allowance: |
$ (5) |
| Total revenue: |
$75 |
You must state your actual charge as revenue and then show your contractual allowances. You cannot just show the difference (ie, $75). This is an accounting rule that only accountants understand!
- Charity and bad debt are similar to contractual allowances except that they are not planned for as in a contract. Charity is a discount that you determine you will give prior to providing the service. Example: You can decide to give a 10% charity write-off to a patient who has limited financial resources. The amount the patient would actually pay of the $80 charge would be $72.
Bad debts are unplanned write-offs from what you had expected to receive for your services. Example: You billed a patient the $80 fee and he or she paid only $40 and never paid any more. After a period of time, you determine that this patient will never pay the remaining amount, and you write it off to bad debt.
Bad debt and charity write-offs are expressed on the income statement:
| Revenue (2 visits): |
$160 |
| Less charity of 10% for 1 visit: |
$ (8) |
| Less bad debt: |
$ (40) |
| Total revenue: |
$132 |
- Depreciation is the financial representation of the normal wear and tear on a large piece of equipment or property determined by taking the total value of the equipment or property and dividing it over a given number of years. This is also referred to as amortizing. The number of years is determined in many ways; the best thing to do is ask the accountant how many years to depreciate each piece of equipment you will need. Most organizations choose a specific dollar amount over which they will depreciate an item. Example: Anything over $500 or sometimes $1000 will be depreciated.
Example: You will need a biofeedback machine for your incontinence clinic that will cost $10,000. The accountant tells you that it will need to be depreciated over 5 years. The amount that will be “expensed” each year is $2000 ($10,000 divided by 5). The tricky part here is that the actual cash ($10,000) for the equipment will be spent when the equipment is purchased. However, the IRS will only let you recognize $2000 in expenses per year. In your pro forma budget, you will record an expense of $2000 each year for 5 years.
- When determining the costs that must be considered for your business/product, you will need to decide which are fixed and which are variable costs. Fixed costs are those costs that do not vary with the amount of services you provide. Example: Rent and depreciation on equipment are fixed. If your rent is $1000 per month, it does not matter whether you see 5 patients or 50 patients, the rent will not change. Variable costs are those costs that vary with the amount of services provided. Example: Patient care staff salaries and supplies will vary with the number of patients. You will use more supplies to see 50 patients than you will to see 5 patients.
- The importance of understanding fixed and variable costs is that you can control variable costs much more easily than you can control fixed costs. Frequently, you are more valuable to an organization as a variable cost than you are as a fixed cost. If you are a full-time employee with a set salary and benefits, you are a fixed cost. Whether you see 100 patients or 1000 patients, your salary and benefits will cost the organization the same. However, if you have a contract for a per unit fee, you are a variable cost. If your per unit fee is $75, the total amount the organization pays will vary with the number of units of service you provide. Therefore, if business is slow for your client (eg, a hospital), they can pay you for just the number of visits or amount of service that they need. When business is better, they are able to pay you for increased amounts of service.
The Budgeting Process
Now that you understand a few of the basic concepts, you are ready to begin collecting data for the pro forma budget. You must determine how much total revenue by source and total expenses by source you expect.
To determine the revenues and expenses, certain exercises are necessary:
- Statistical forecasting—trending
This is how you can determine the expected revenues for your business/product. If it is an existing business/product, you can use past data to forecast the coming year(s). If it is a new business/product, you will use your situation and market analyses to project the future years. This part of forecasting is based on utilization only. Example: You will determine the number of patients, procedures, visits, hours, and so forth, that you will provide. The unit to use is based on the mechanism by which you are paid. Example: If you are paid for the service by hour, you should project in hours, and so forth.
- Example:
| Patient Visits |
'10 |
'11 |
'12 |
% Forecast∗ |
'13 Projected |
| Ostomy |
500 |
460 |
440 |
3% |
426 |
| Wounds |
800 |
1000 |
1300 |
20% |
1560 |
| Continence |
300 |
550 |
700 |
30% |
910 |
| Total: |
1600 |
2010 |
2440 |
19% |
2896 |
| ∗The forecast is calculated by averaging the % of increase for each of the past 3 years and then estimating any additional increase or decrease based on market factors. |
- Based on your analyses, complete the following chart:
| |
For Existing Businesses/Products |
For All Businesses/Products |
| Revenue Source |
Prior Year 1 |
Prior Year 2 |
Prior Year 3 |
Percent Forecast |
Projected Year 1 |
Projected Year 2 |
Projected Year 3 |
| Ostomy |
N/A |
N/A |
N/A |
N/A |
300 |
330 |
350 |
| Wound |
N/A |
N/A |
N/A |
N/A |
1000 |
1100 |
1600 |
| Continence |
N/A |
N/A |
N/A |
N/A |
400 |
440 |
500 |
| Miscellaneous hourly consults |
N/A |
N/A |
N/A |
N/A |
100 |
110 |
175 |
| Total |
|
|
|
|
1800 |
1980 |
2625 |
- Expense forecasting
Now, you will begin to think in dollar amounts. You will need to list all of your expenses and do the same type of trending that you did in the statistical forecasting.
Expenses that you should consider are as follows:
- Salaries/benefits—of all personnel (including yourself) involved in the business/product. You will need to know how much time will be worked and the salaries and benefits of each individual.
- Taxes and other employee expenses—the accountant can provide this information.
- Rent.
- Supplies/equipment—this includes only the supplies and equipment that will not be depreciated. You can also include your brochures, business cards, and office supplies here. Repairs on equipment can be included here also.
- Depreciation∗—this is where the $2000 of depreciation for the biofeedback machine in the example would be noted.
- Professional fees—this would include your outside advisors such as accountants, attorneys, and so forth.
- Dues/membership—you can include any professional journal subscriptions or memberships to professional organizations in this category.
- Education—this would include any seminars or conferences that you plan on attending. Expenses in this category include flight, mileage, food, lodging, and so forth, related to the educational event.
- Travel—these are travel costs associated with providing the service.
- Postage and shipping.
- Utilities—this would include phone, electric, gas, and so forth.
- Marketing/advertising—include any media that you will be using. This could be online marketing, telephone book listings, advertising, and other expenses associated with marketing. If you did not include your business cards and/or brochures under supplies, you could put them here.
- Miscellaneous—anything that cannot be reasonably classed in the aforementioned categories could be included here.
______________________________________________________________________________________________________________________
∗To determine your depreciation amount, you will need to list the “capital equipment” you need. Capital equipment is equipment that is over the depreciable limit set by you or the organization (usually $500 or $1000). Remember to ask the accountant about how many years the equipment needs to be depreciated.
- What depreciable equipment will you need?
| Equipment |
Cost |
Purchase Date |
Depreciable Years |
| Computer |
$2000 |
June |
5 |
| Printer |
$600 |
June |
5 |
| Copier |
$1000 |
June |
5 |
Again, if it is an existing business/product, you can use previous data to forecast; if it is a new business/product, you must use your best educated guess.
- Example:
| Expenses |
'10 |
'11 |
'12 |
% Forecast∗ |
'13 Projected |
| Salaries |
$50 |
$52.50 |
$80 |
38 |
110.40 |
| Rent |
$12 |
$12.60 |
$13.20 |
5 |
$13.80 |
| Other |
$20 |
$22 |
$25 |
0 |
$25 |
| Total |
$82 |
$87.10 |
$118.20 |
26 |
$149.40 |
| ∗The forecast is calculated by averaging the % of increase for each of the past 3 years and then estimating any additional increase or decrease based on market factors. |
- Complete the following chart to determine your projected expenses:
| |
For Existing Businesses/Products |
For All Businesses/Products |
| Expense Source |
Prior Year 1 |
Prior Year 2 |
Prior Year 3 |
% Forecast |
Projected Year 1 |
Projected Year 2 |
Projected Year 3 |
| Salaries |
N/A |
|
|
|
$110,000 |
$115,000 |
$141,275 |
| Taxes/employee expense |
|
|
|
|
$3,250 |
$3,350 |
$4,450 |
| Rent |
|
|
|
N/A |
$1,000 |
$1,100 |
$1,200 |
| Supplies/equipment |
|
|
|
|
$2,500 |
$1,000 |
$1,000 |
| Depreciation |
|
|
|
|
$360 |
$720 |
$720 |
| Professional fees |
|
|
|
|
$1,000 |
$750 |
$500 |
| Dues/members |
|
|
|
|
$150 |
$150 |
$150 |
| Education |
|
|
|
|
$1,200 |
$1,200 |
$2,400 |
| Travel |
|
|
|
|
$4,000 |
$4,400 |
$2,400 |
| Postage |
|
|
|
|
$250 |
$100 |
$4,840 |
| Utilities |
|
|
|
|
$600 |
$700 |
$100 |
| Marketing |
|
|
|
|
$1,500 |
$750 |
$750 |
| Total |
|
|
|
|
$125,810 |
$129,720 |
$158,085 |
- Cost per unit
- The next step is to determine the average cost per unit based on your projections. It is calculated as follows:
- Average cost/unit = All expenses divided by the number of units
- Example: $149,400 ÷ 2896 = $52 per visit
- From your charts above, fill in the blanks to determine your projected average cost per unit for each year.
- Year 1:
Total expenses $125,810 ÷ Total number of units 1800 = $70 per unit
- Year 2:
Total expenses $129,720 ÷ Total number of units 1980 = $65.50 per unit
- Year 3:
Total expenses $158,085 ÷ Total number of units 2625 = $60.25 per unit
- Revenue forecast
Forecasting revenue is more difficult than forecasting expenses. There is no set rule for what your charge should be. Consideration must be given to what is charged for similar services, what the competition is charging, and what the market will bear. Wound, Ostomy and Continence Nurses Society compiled a salary and productivity survey of members in 2008. This beneficial tool can help you determine your fee for service based on your geographical location or expertise (WOCN, 2008).
- Table 1: Typical Hourly Rate for Contractual Services
| Setting |
Number of Respondents |
Median |
Average |
25th Percentile |
75th Percentile |
| Acute care |
28 |
$67.50 |
$73.82 |
$56.88 |
$81.25 |
| Home care |
34 |
$65 |
$66.91 |
$53.13 |
$80 |
| Subacute |
14 |
$65 |
$61.25 |
$50 |
$78.75 |
| Long-term care |
34 |
$65 |
$68.63 |
$50 |
$80 |
| Outpatient/wound care center |
13 |
$55 |
$63.40 |
$52 |
$65 |
| Education |
29 |
$77.50 |
$74.98 |
$50 |
$100 |
| Expert chart review |
22 |
$162.50 |
$164.80 |
$125 |
$200 |
| Depositions |
14 |
$250 |
$274.69 |
$200 |
$400 |
| Protocol development |
16 |
$77.50 |
$81.53 |
$45 |
$100 |
| Workshop |
20 |
$100 |
$129.47 |
$54.38 |
$150 |
If you have the luxury of using your charge in all cases, use the average cost per unit that you just calculated and add on an appropriate profit. If you have contracted rates that are different than your charge, you must consider the difference between your charge and the contracted rate. You will, however, most likely be charging different prices for different types of services.
- Example:
| Revenue Source |
Average Revenue/Unit |
Number of Visits |
Total $ |
| Ostomy |
$60 |
426 |
$25,560 |
| Wounds |
$72 |
1,560 |
$112,320 |
| Continence |
$78 |
910 |
$70,980 |
| Total |
|
|
$208,860 |
- Determine your expected revenue by completing the following charts:
- Year 1:
| Revenue Source |
Revenue per Unit |
Number of Units |
Total Revenue |
| Ostomy |
$70 |
300 |
$21,000 |
| Wound |
$75 |
1000 |
$75,000 |
| Continence |
$75 |
400 |
$30,000 |
| Consulting |
$90 |
100 |
$9,000 |
| Total |
Average: $75 |
1800 |
$135,000 |
If you have the luxury of using your charge in all cases, use the average cost per unit that you just calculated and add on an appropriate profit. If you have contracted rates that are different than your charge, you must consider the difference between your charge and the contracted rate. You will, however, most likely be charging different prices for different types of services.
- Year 2:
| Revenue Source |
Revenue per Unit |
Number of Units |
Total Revenue |
| Ostomy |
$70 |
330 |
$23,100 |
| Wound |
$75 |
1100 |
$82,500 |
| Continence |
$75 |
440 |
$33,000 |
| Consulting |
$90 |
110 |
$9,900 |
| Total |
Average: $75 |
1980 |
$148,500 |
- Year 3:
| Revenue Source |
Revenue per Unit |
Number of Units |
Total Revenue |
| Ostomy |
$70 |
350 |
$24,500 |
| Wound |
$75 |
1600 |
$120,000 |
| Continence |
$75 |
500 |
$37,500 |
| Consulting |
$90 |
175 |
$15,750 |
| Total |
Average: $75 |
2625 |
$197,750 |
- Break-even analysis
- The break-even analysis is important in determining how many units of service you need to provide in order to cover your expenses. It is calculated as follows:
- Average revenue/unit × Number of units = Total expenses
- Example: $70 × Number of units = $149,400
Number of units = $149,400 ÷ $70
Number of units = 2134
This means that 2134 visits are needed to cover expenses. It is not unusual for a new business/product to lose money the first year or so; however, you need to project when you expect to break even and then start making a profit. During the years that you will be breaking even or losing, you need to have financial support to at least pay your bills.
- Calculate your estimated break-even point:
- Pro-forma income statement
Believe it or not, this is the easiest part. Very simply put, the pro forma income statement indicates the revenue minus expenses—information you have already calculated. It finally shows you what your “bottom line” will be over the next 3 years.
- Example: For the simple example that we have been following, the net income will be: $208,860 – $149,400 = $59,460
For the body of the business plan, you need only include the abbreviated financial analysis. Save all the details for the Appendix.
- Summarize your pro forma results: See appendix for detailed financial statements.
Summary:
- Year 1:
Total revenue $135,000 – Total expenses $125,810 = $9190
- Year 2:
Total revenue $148,500 – Total expenses $129,720 = $18,780
- Year 3:
Total revenue $197,750 – Total expenses $158,085 = $39,665
Appendix S–II: Sample Business Plan: Always Wright Consulting Services
Always Wright Consulting Services
April 30, 2011
Contact person:
Kristy Wright, MBA, RN, CWOCN
1234 Maple Lane
Anywhere, PA 10023
(555) 123-4567
Table of Contents
Executive Summary
Present Situation
Goals and Objectives
Business/Product Description
Critical Success Factors and Key Assumptions
Always Wright Consulting Services Staffing Structure
Proposed 2012 Budget
Contractual Agreement
Appendices (Note: Sample items are not included here but would be included in an actual proposal.)
Executive Summary
Always Wright Consulting Services (AWCS) is a professional nursing and organizational development firm that will provide clinical wound, ostomy and continence (WOC) services and assist with development of programs, clinics, protocols, outcome data, and regulatory compliance. AWCS is also expert in reimbursement issues.
In the proposed service area, the 5 diseases causing the highest incidences of mortality and morbidity are directly related to the service capability of AWCS. They include diabetes, cancer, circulatory disorders, and accidents. One city in the area has a particularly high incidence of bladder cancer with resultant cystectomy. In addition, due to the concentration of the elderly, there is a relatively high incidence of untreated incontinence. The long-term care facilities in the area feel that it is their greatest concern followed closely by pressure ulcers. AWCS will address the most costly physical manifestations of the aforementioned diseases that would express themselves in wounds, chronic peripheral vascular ulcers, incontinence, and ostomies.
In the current competitive managed care environment, health care organizations need to provide quality services in a cost-effective and efficient manner. The obvious benefit of utilizing AWCS is an improvement in the quality of life for patients. AWCS ensures this through individualized patient education, continuity of care across all settings, family involvement, decreased complications, and a more rapid return to normal activities. AWCS will benefit the contracting customer (organization) through cost savings by managing resources, ensuring that services and supplies are reimbursable, treating the patient in the most effective setting, reducing length of stay, and decreasing complications and readmissions. In addition, AWCS will assist with regulatory compliance through staff education, protocol development, outcome data collection, and quality measurement. These benefits will give the customers a competitive advantage and put them in a solid position to work with managed care organizations and negotiate for capitated contracts.
AWCS will serve a variety of customers and consumers, each with different characteristics and needs. Service delivery will remain flexible in order to target the needs of each customer group. A specific plan has been developed for each customer segment that includes customer characteristics, the “message” that needs to be conveyed to each customer, and strategies for improving customer relations.
The long-range goal is to financially break even by the end of the second year of business. In order to achieve this, the following goals have been established:
- Achieve a 10% to 15% growth over each of the next 5 years.
- Pay off start-up debt in 5 years.
- Realize a profit in 2 years.
- Ensure quality services with measured outcomes.
- Employ qualified team members.
The success of AWCS is reliant on certain critical success factors. AWCS must acquire certain resources in order to achieve a successful and profitable business within the time frame stated in AWCS goals. Resources needed include personnel, equipment and supplies, and start-up capital. AWCS must also secure at least 2 hospital contracts prior to beginning business.
The current environment is exciting and promising for AWCS to begin business. Once established, the firm has plans to grow and expand in size, available services, and geographic area. The current partners are certified in WOC nursing. Plans are in place to hire additional professional staff as the business grows.
Present Situation
The current environment for this new business is very exciting. Managed care is increasing penetration into all health care settings in western Pennsylvania. Many of the smaller hospitals and alternative settings are merging or affiliating to form larger networks. The challenge is to reduce costs, maintain quality, and learn how to work cooperatively with managed care organizations.
External Analysis
The population in the area has an average age of 73 years, and the fastest growing age group is older than 80 years. Although the average income is relatively low ($25,000/y), the elderly population creates many opportunities for services by AWCS.
The 5 diseases causing the highest incidences of mortality and morbidity are directly related to the service capability of AWCS. They include diabetes, cancer, circulatory disorders, and accidents. One city in the service area has a particularly high incidence of bladder cancer with resultant cystectomy. In addition, due to the concentration of elderly in the area, there is a relatively high incidence of untreated incontinence. The long-term care facilities in the area feel that it is their greatest concern followed closely by pressure ulcers. AWCS will address the most costly physical manifestations of the aforementioned diseases, which would express themselves in wounds, chronic peripheral vascular ulcers, incontinence, and ostomies.
Competitive Analysis
There is moderate competition in the service area. Two other WOC nurses are in practice; however, both work full-time for acute facilities. Physical therapists and 1 physician's group also provide wound care on an inpatient and outpatient basis.
The primary competitive concern is that physical therapists and the physician group receive direct Medicare reimbursement for their services. It is unlikely that Medicare will revise payment regulations to include WOC nursing. Therefore, AWCS will need to present their services to customers from a cost-savings perspective.
AWCS has an edge over competitors by offering a comprehensive service that includes not only clinical care but also organizational development. This allows AWCS to provide protocol development, business development (including outpatient clinics), marketing to managed care, and assistance with reimbursement.
Internal Analysis
AWCS has the ability to provide expert WOC care in all settings. The staff possesses a variety of clinical skills and certifications including special expertise in delivering care in the patient's home. In order to fully meet the demands of potential customers, the company will need to collect outcomes data to present to organizational customers (including managed care). In addition to clinical expertise, AWCS has a unique strength in other related business skills, including organizational development, reimbursement issues, financial analysis, marketing, and medical equipment management. In order to work within the managed care environment, knowledge and skill with capitation will need to be developed.
Financially, the company has obtained a small business loan, has $5000 in start-up cash, and has 2 guaranteed contracts. Although total income is uncertain, the AWCS could remain financially solvent through the first 2 years.
Goals and Objectives
AWCS planned on beginning business on September 1, 2011, as a partnership. The long-range goal was to financially break even by the end of the second year of business and then to add other staff. In order to achieve this long-range plan, the following goals have been established:
- Achieve a 10% to 15% growth over each of the next 5 years.
- Pay off start-up debt in 5 years.
- Realize a profit in 2 years.
- Ensure quality services with measured outcomes.
- Employ qualified team members.
The following objectives have been developed to meet AWCS's goals:
Goal 1: Achieve a 10% to 15% growth over each of the next 5 years.
| Steps to Achieve |
Resources Needed |
Completion Date |
| Get contract with 2 hospitals |
None additional |
December 2012 |
| Get contract with 3 home care organizations |
Possibly half-time WOC nurse funding, staffing, van, equipment |
March 2013 |
| Establish outpatient clinic |
Funding, staffing, space |
December 2015 |
| Establish mobile clinic |
Funding, staffing van, equipment |
December 2016 |
Goal 2: Pay off start-up debt in 5 years.
| Steps to Achieve |
Resources Needed |
Completion Date |
| Put 5% of revenue toward loans each quarter |
Adequate revenue |
Each quarter, ending in 2016 |
Goal 3: Realize a profit in 2 years.
| Steps to Achieve |
Resources Needed |
Completion Date |
| Get contract with 2 hospitals |
None additional |
December 2012 |
| Get contract with 3 home care organizations |
Possibly half-time WOC nurse funding, staffing, van, equipment |
March 2013 |
Goal 4: Ensure quality services with measured outcomes.
| Steps to Achieve |
Resources Needed |
Completion Date |
| Develop clinical guidelines for practice |
Wound, Ostomy and Continence Nurses guidelines |
December 2012 |
| Set up database to collect outcome data |
Education for secretary on database management |
March 2013 |
| Analyze and report data |
Time!!! |
September 2013 |
Goal 5: Employ qualified team members.
| Steps to Achieve |
Resources Needed |
Completion Date |
| WOC nurses to attend Wound, Ostomy and Continence Nurses conferences |
Funding and patient coverage |
Annually |
| WOC nurses to be certified |
Funding |
Every 5 years |
| Database management education for secretary |
Funding and time |
March 2013 |
Business/Product Description
AWCS will provide comprehensive clinical, business, and development services that include the following:
- Clinical services and consultation
- Comprehensive management of patients with wounds, ostomies, and incontinence
- Assessment
- Prevention
- Patient education
- Treatment selection and implementation
- Case management
- Care coordination
- Resource utilization
- Continuity
- Patient advocacy
- Long-term management
- Education and development
- Protocol development
- Staff education
- Program development (ie, outpatient clinics, etc)
- Regulatory compliance
- Research
- Clinical trials
- Outcome data
The obvious benefit of utilizing AWCS is an improvement in the quality of life for patients. AWCS ensures this through individualized patient education, continuity of care across all settings, family involvement, decreased complications, and a more rapid return to normal activities. AWCS will benefit the contracting customer (organization) through cost savings by managing resources, ensuring that services and supplies are reimbursable, treating the patient in the most effective setting, reducing length of stay, and decreasing complications and readmissions. In addition, AWCS will assist with regulatory compliance through staff education, protocol development, outcome data collection, and quality measurement. These benefits will give the customers a competitive advantage and put them in a solid position to work with managed care organizations and negotiate for capitated contracts.
Most importantly, in the current economic environment of health care, contracting for services is a variable rather than fixed cost. This allows the customer to have “just in time” service without the overhead costs associated with employee downtime and fluctuations in productivity.
“Quick Referral” System
AWCS has developed a “Quick Referral” system to streamline access to services. Referral forms will be provided to each customer on disk and in hard copy. Written referrals may be faxed 24 hours a day or e-mailed to [email protected]. In addition, referrals can be called directly to the office from 8 am to 5 pm or to the 24-hour answering service. AWCS also has 24-hour on call staffing for emergencies.
Service Area
- AWCS provides the full range of services to the following areas:
- Butler County
- Armstrong County
- Lawrence County
- Alle-Kiski Valley area
Critical Success Factors and Key Assumptions
AWCS will require certain resources to be in place in order to achieve a successful and profitable business within the time frame discussed in the AWCS goals. Resources needed include the following:
Personnel
- Administrator
- Two clinical staff (certified WOC nurses)
- One secretary/receptionist
Equipment
- Office space to accommodate the clinical staff and administrative personnel
- At least 3 phones and phone lines (1 dedicated to fax/modem)
- Two computers (with built-in fax/modem capabilities)
- Two printers
- Copy machine
- E-mail and Internet service
Capital
Always Wright Consulting Services
Contractual Agreement
Contractual Agreement Between ABC Agency and Sarah Smith, BSN, RN, CWOCN
(Note: Usually begins with introductory paragraph explaining the purpose of the contract.)
Purpose
Whereas ABC Agency (hereinafter referred to as “Agency”) desires to assure the provision of outcomes-oriented and cost-effective care to its patients with compromised skin integrity, chronic wounds, ostomies, or incontinence, and Sarah Smith, BSN, RN, CWOCN (hereinafter referred to as WOC nurse), desires to provide these services on a contractual basis, these parties hereby enter into this contractual agreement.
May include general background information regarding scope of practice and qualifications.
Background
The WOC nurse is minimally a baccalaureate-prepared RN who has graduated from a nationally accredited program in wound, ostomy and continence (WOC) nursing. The designation CWOCN reflects National Board Certification by the Wound, Ostomy and Continence Nursing Certification Board and is a nationally recognized measure of current knowledge and competence in the field of WOC nursing.
The WOC nurse scope of practice includes the following:
- Assessment and early intervention for patients at risk for skin breakdown.
- Outcomes-oriented management of chronic wounds such as pressure ulcers and lower extremity ulcers.
- Rehabilitative care for patients with ostomies or continent diversions.
- Cost-effective management of chronic percutaneous tubes, draining wounds, and fistulas.
- Implementation of effective bowel and bladder programs to correct or manage urinary and/or fecal incontinence.
The contract should include specific responsibilities of each party. See the following example:
Specific Responsibilities of WOC Nurse:
- WOC nurse agrees to provide the following patient care services upon consultation:
Wound Care:
- Assessment of etiologic factors with recommendations for correction.
- Baseline assessment of systemic factors impacting on healing, with recommendations for further assessment/intervention as needed.
- Assessment of wound status and recommendations for topical therapy.
- Conservative sharp wound debridement when indicated (and with MD order).
- AgNO3 cauterization of hypertrophic granulation tissue and/or nonproliferative wound edges when indicated.
- Recommendations for referral when indicated.
- Establishment of effective pouching system for patient with draining wound or fistula.
Ostomy Care:
- Preoperative teaching and stoma site marking.
- Postoperative assessment of stoma, output, and pouching surface; selection of appropriate pouching system.
- Patient and family education regarding ostomy management.
- Patient counseling to facilitate adaptation and resumption of preoperative lifestyle.
Continence Care:
- Assessment of etiologic factors, patterns of incontinence, and potential for restoration of continence.
- Recommendations for referral when indicated.
- Recommendations for management to include bowel and bladder training programs; toileting programs; instruction in clean intermittent catheterization; instruction in pelvic muscle exercises; and appropriate use of devices, absorptive products, and skin care products.
- WOC nurse agrees to respond to consult within 24 working hours unless alternate arrangements are made.
- WOC nurse agrees to obtain MD orders for all care provided and to communicate all care recommendations to staff and MD via written documentation on the progress notes and the plan of care and verbal communication to the staff.
- WOC nurse agrees to provide in-services to staff within areas of expertise upon request and within mutually agreed upon parameters regarding length, content, materials to be provided, program dates, and compensation.
- WOC nurse agrees to maintain current registration as RN within state of __________ and current board certification as WOC nurse, with documentation provided to Agency upon request.
- WOC nurse agrees to maintain own professional liability insurance with minimum of $1 million per incident and $3 million aggregate coverage and to make documentation of coverage available to Agency upon request.
- WOC nurse agrees to provide documentation of acceptable health status to Agency (to included negative PPD updated every 6 months; immunity to measles, mumps, and chicken pox documented by titers or by immunizations × 2; immunity to hepatitis B documented by titers or by evidence of HeptaVax × 3, or signed statement of declination and acceptance of responsibility).
- WOC nurse agrees to submit monthly invoice to Agency for services provided; invoice for each month of services will be submitted by the 15th of the following month along with itemized statement delineating services provided.
- WOC nurse agrees to pay own federal, state, and social security taxes.
Specific Responsibilities of Agency:
- Agency agrees to provide WOC nurse with staff privileges and to orient WOC nurse to agency.
- Agency agrees to appoint a contract person and supervisor for the WOC nurse.
- Agency agrees to notify the medical staff and nursing staff in writing of the appointment of the WOC nurse to the Agency's consultant staff; such notification shall be accompanied by the following:
- List of specific services provided (as outlined in Item 1 of previous section “Specific Responsibilities of WOC Nurse”).
- Guidelines for initiating a consult.
- Relevant agreements, that is, time frame for WOC nurse's response to a consult, WOC nurse's responsibility for obtaining any needed orders, WOC nurse's communication with staff, and documentation on patient record.
- Agency agrees to notify WOC nurse by beeper (beeper #) of patients to be seen and reason for consult.
- Agency agrees to handle all patient billing.
- Agency agrees to remit payment for services provided within 4 weeks following receipt of invoice. Payment shall be made according to the attached fee schedule. Would need to attach a fee schedule; see fact sheet on contractual agreements for tips.
- Agency agrees to provide institutional liability coverage for WOC nurse services.
- Agency agrees to provide free parking to WOC nurse.
- Agency agrees to provide all patient care supplies required for WOC care.
Joint Responsibilities:
- Both parties agree to hold an evaluation conference annually to review the services being provided and to resolve any issues or problems. In addition, each party agrees to meet at any time upon the second party's request to discuss and resolve any issues.
- This agreement may be terminated at any time by mutual consent or by either party with written notification of the second party; such notification must be made 60 days prior to the termination date.
- This agreement is effective________________________________
________________________ ________________________
Agency representative Provider
Appendix S–III: A Business Financial Glossary
Account payable—A liability representing an amount owed to a creditor, usually arising from purchase of merchandise or materials and supplies. Normally a current liability.
Account receivable—A claim against a debtor usually arising from sales or service rendered. Normally a current asset.
Accrual basis of accounting—The method of recognizing revenues as goods that are sold or services that are rendered, independent of the time when cash is received. Expenses are recognized in the period when the related revenue is recognized, independent of the time when cash is paid out.
Asset—A resource with exchange or economic value.
Bad debt—An uncollectible account receivable.
Balance sheet—A financial report that profiles the economic condition of an organization as of a moment in time.
Budget—A financial plan used to estimate results of future revenues and expenditures.
Capital budget—Plan of proposed outlays for acquiring long-term assets and the means of financing the acquisition.
Cash—Currency and coins, negotiable checks, and balances in bank accounts.
Current assets—Cash and other assets that are expected to be turned into cash, sold, or exchanged within the normal operating cycle of the firm, usually 1 year. Current assets include cash, receivables, and inventory.
Depreciation—An expense that represents the normal wear or deterioration experienced by an asset.
Direct costs—Costs that can be identified with and that result from the production of a specific good or delivery of a specific service.
Expense—Use of assets in producing revenue or carrying out other activities that are part of operations.
Fixed cost—An expense that does not vary with volume of goods or services produced.
GAAP—Generally accepted accounting principles.
Income—Excess of revenues over expenses. Also referred to as net income.
Income statement—Financial statement of revenues, expenses, and net income.
Indirect costs—Costs of production not easily associated with the production of specific goods or services. Also referred to as overhead.
Liability—Financial responsibilities and debts resulting from current operations and investment in fixed assets.
Long-term debt—Debt or liability that will typically be repaid over a period greater than 1 year. This debt is usually acquired in obtaining fixed assets.
Net income—See income.
Overhead—Any cost not associated directly with the production of goods or services. Also referred to as indirect costs.
Pro forma—Hypothetical financial statements as they would appear if some event such as a merger, increased production, or addition of a new service had occurred. Frequently done in the form of a pro forma budget.
Revenue—The monetary measure of a service rendered or goods sold.
Variable costs—Expenses that vary with the volume of goods produced or services rendered.
References
Grossman, S., & Valiga, T. (2005). The new leadership challenge: Creating the future of nursing (2nd ed.). Philadelphia, PA: F. A. Davis Company.
Marquis, B., & Huston, C. (2006) Leadership roles and management functions in nursing: Theory and application (5th ed.) Philadelphia, PA: Lippincott Williams & Wilkins.
Wound, Ostomy and Continence Nurses Society (2008). WOCN salary and productivity survey. Retrieved November 19, 2010, from http://www.wocn.org
Wound, Ostomy and Continence Nurses Society (2010). Wound, ostomy and continence nursing scope & standards of practice. Mt. Laurel, NJ: Author.
Appendix T: Sample WOCN Society Member's Research Grant Proposal∗
∗Note: The following is an example of a research grant proposal provided by the Center for Clinical Investigation (CCI) of the Wound, Ostomy and Continence Nurses Society Foundation. This document was developed by the CCI and is available at the WOCN Web site (http://www.wocn.org/ResearchFunding). The document is provided here only as an example and is subject to change. Please contact CCI or check the Web site to verify current funding opportunities and the proposal process.
Funding Priorities:
WOCN Society Member's Research Grant—$10,000:
Any topic of WOC nursing practice that promotes the science or practice of the WOC nursing specialty.
This grant proposal is divided into 4 sections:
- Grant Submission Instructions
- Title Page
- Proposal Guide
- Checklist
- GRANT SUBMISSION INSTRUCTIONS
- Notice of interest
- Please submit a Notice of Interest e-mail to Linda Dahle, Program Associate ([email protected]) when you are considering applying for a Member's Research Grant. This is not a commitment, and you can notify CCI later if you change your mind. This will enable CCI to send you any updates or resources to assist you. Please include the following information in the Notice of Interest e-mail:
- Principal investigator's (PI) name
- Topic you are considering studying and the title of proposal
- A statement of the purpose of the study
- E-mail address
- Telephone number
- The title page to be completed includes the following information:
- Title of research grant
- Principal investigator's name
- Academic degrees
- Current professional certification
- Home address
- Current employer
- Employer address
- Preferred mailing address
- Work/home telephone numbers
- Fax number
- E-mail
- Registered nurse/license number/state of PI and Co-PI
- WOCN Society Co-I Member Number of PI and Co-PI
If you have team members as part of your study, please fill out,“Other Team Members Contact Information” (please copy table on separate pages for as many team members as you have).
- The following sections are included in the Proposal Guide, and need to be completed in order to be considered for funding:
A) Title Page
B) Abstract (summary of proposal)
C) Scientific Plan (statement of problem including fit with grant and relevance to WOC nursing, research questions/aims, review of literature, references, methods)
D) Bio-sketch of Principal Investigator (PI)
E) Co-Investigator(s) Bio-sketch
F) Statement of Team Qualifications/Strengths
G) Project Budget
H) Budget Justification
I) Human Subjects/Ethical Considerations
J) Timeline
K) Scientific and Funding Overlap—Duplicative funding will not be accepted (ie, funding for same project by more than 1 grant). Please see the “K. Scientific and Funding Overlap” section for more detail.
L) Receipt of Funds
M) Appendix (Letters from research mentor; permission of holder of any records to be used, administrative approval to conduct study in an agency, etc, are required)
Research proposal preparation
- The Scientific Plan of the research proposal is a maximum of 10 typed pages in length single space (see Section C), but does not include the abstract, references, biographical sketches, budget, human subjects/ethical considerations, timeline, and other appendix materials.
- Submission content must be:
- Typed single space—maximum 10 pages (references should also be single spaced)
- Leave 1-inch margins on all sides
- Use a 12-point font Arial
- Number every page
- Do not use proportional spacing or justified margins
- One Microsoft Word document that includes ALL the sections of the proposal will be accepted—no PDFs will be accepted.
- The institutional review board (IRB) approval is not required at the time of submission, but an IRB application must be submitted within 30 days of award.
- References
- The authors are responsible for the accuracy of the References. References should use an established format such as in the AMA Manual of Style, 9th ed (p. 43), or Publication Manual of the American Psychological Association (6th ed).
- Submission of a grant proposal:
- E-mail the completed grant proposal by _________Date__________ to:
Linda Dahle, Program Associate: [email protected]
- Questions?
If you have questions about your proposal submission, please contact Linda Dahle at [email protected] or 612.625.8159. If you have any scientific questions, please contact Dr Donna Bliss, Director of the Center for Clinical Investigation, at [email protected].
- TITLE PAGE
- WOCN Society Member's Research Grant—$10,000: Funding priorities: Any topic of WOC nursing practice or that promotes WOC nursing specialty practice.
| ▪ Title of Research Project: |
|
| ▪ Principal Investigator's Name: |
|
| ▪ Academic Degrees: |
|
| ▪ Current Professional Certification: |
|
| ▪ Home Address: |
|
| ▪ Current Employer: |
|
| ▪ Employer Address: |
|
| ▪ Preferred Mailing Address: |
|
| ▪ Home Number: |
|
| ▪ Fax Number: |
|
| ▪ PI's Registered Nurse License Number/State: |
|
| ▪ Co-PI's Registered Nurse License Number/State (if applicable): |
|
| ▪ PI's WOCN Member Number: |
|
| ▪ Co-PI's WOCN Society Member Number (if applicable): |
|
- OTHER TEAM MEMBERS' CONTACT INFORMATION
(Please copy table on separate pages for as many team members as you have.)
| Role |
Name |
Credentials |
Work Affiliation |
Responsibilities/Contributions to Study |
Address |
Telephone/E-mail Address |
| Co-Investigator(s) |
|
|
|
|
|
|
| Research Mentor |
|
|
|
|
|
|
| Statistician |
|
|
|
|
|
|
| Consultant |
|
|
|
|
|
|
| Other |
|
|
|
|
|
|
- PROPOSAL GUIDE
- COMPLETE TITLE PAGE
- ABSTRACT (250-300 words maximum). The abstract is a summary of the entire proposal written in lay language. The abstract needs to include significance, purpose, research questions, aims, design, sample and summary of main procedures, planned statistical analyses, and expected outcomes.
- SCIENTIFIC PLAN—No more than 10 pages single space in length maximum, and include the following 4 areas:
- Statement of the Problem: includes significance, innovation of study, and how you meet priority of the grant (approximately 1–2 pages). Opening sentences should communicate what the study is about. Be succinct, clear, and direct.
a) Significance:
- What is this study about?
- Why is the topic important?
- What new knowledge will your study offer?
- Is it timely?
- What is its relevance to WOC nursing?
- What is the clinical or scientific problem and need for your study?
- Support with statistics, epidemiology.
- Expert opinion.
- Formal position/white papers of societies.
b) Innovation of Study:
- Explain what is unique or new about the study.
- Are you bringing 2 ideas together in an innovative way?
- Are you proposing a new way of thinking?
- Are you proposing a new solution to an existing problem?
- Are you proposing a novel approach of studying problem?
c) Priority areas of grant:
- How do your priority areas fit with the priority areas of the grant?
- Research Questions/Aims:
- 1/2 page in length
- Questions you will answer (2–3 questions is usually enough).
- Statements of what you intend to do and accomplish.
- Make known your main variables, sample, study design.
- Must be measurable outcomes.
- Be clear.
- Not too broad—must be measurable.
- Not too narrow—must be relevant.
- Not too complicated—must be understandable.
- Not too simplistic—must be important.
- Should be specific, not general or ambiguous.
- Review of Literature
- 2 to 3 pages in length
- Critique quality of key individual studies.
- Do not just describe—why is your study better/needed than what is published?
- Evaluate state of science/evidence base.
- Interpret conflicting information.
- Demonstrate knowledge about the problem and area of science
- Identify the GAPS in knowledge that your study will address:
- What information is missing that is important to know?
- What new contribution to knowledge will your findings make?
- Has practice or technology changed so that new information from your study is needed?
- Include only most relevant studies.
- Include most current articles and only pivotal historical ones.
- Methods (4-5 pages in length)
a)Design
- Specifically identify the design
- Determined by the research question
- Provides logical link among aims/questions, procedures, and analysis
Question—Design—Methods—Analysis
- Consult a statistician, experienced researcher about best approach
b) Procedures
- How will the proposed research be conducted?
- Address the following:
- Sample—the number and characteristics of subjects to be studied.
- Sampling—strategies for recruiting subjects from where they will be recruited.
- Explain procedures in good detail what you plan to do.
- Describe groups you will form, including any control/placebo groups.
- If doing random assignment, describe how it will be done.
- Indicate points of interaction and data collection with subjects.
- If you will do an intervention, explain what the intervention is, how you will implement it, and the data collection points. Include explanation of any placebo.
- What are the expected outcomes of the study and how will they will measured, what instruments will be used, etc.?
- How will you obtain data? Describe instruments, surveys, etc., that will be used to collect data.
- Address their validity and reliability.
- Potential problems and how you plan to address/avoid them.
c) Analysis
- Describe statistical testing or qualitative analysis as appropriate (frequencies, correlations, chi-square, t tests).
- Appropriate statistical tests or analyses (for research question, type of data, frequencies, correlations, chi-square, t tests).
- Organize by research aim/question.
- Consult a statistician whenever possible.
THE FOLLOWING ARE NOT INCLUDED IN THE 10-PAGE LIMIT:
- BIO-SKETCH OF PRINCIPAL INVESTIGATOR (PI) and Co-PI (2–4 pages)
- An example of a National Institutes of Health biosketch that you can follow is available at: http://grants.nih.gov/grants/funding/2590/biosketchsample.pdf
- A biosketch includes:
- Name and credentials
- Education (post–high school through present; institution, location, dates of attendance, degree, date degree was awarded)
- Professional employment (title of position(s), address of employer, inclusive dates, certifications, and dates)
- Publications
- Any previous research experience (including funded research where you were the investigator, years, funder, and monetary amount of grant; role on other projects or other experience that would support your role as a PI; briefly describe type and level of experience/participation)
- COINVESTIGATOR(S) BIOSKETCH (2–4 pages maximum for each person). List any coinvestigators and attach a biosketch for each that contains information as described for a PI in D. above.
- STATEMENT OF TEAM QUALIFICATIONS/STRENGTHS. (Approximately ½-1 page in length)
Include a statement about the role of each team member on the study, the qualifications and strengths of the research team, whether you have worked effectively together before, and what the consultants (if any) will add, etc.
- PROJECT BUDGET:
In preparing your budget, please address the following categories of items: Supplies, Equipment, Photocopying, Services, Postage, Consultants, Technical Support Staff, Computer-related, Other Costs, and Indirect Institutional Administrative Costs, followed by a Total Amount of Budget Requested (see below).
A few items to note:
- Funds cannot be used as salary support of the PI, Co-PI, or any Co-I or mentor, but can be used to support technical staff, such as statistician or data collector, etc.
- Up to 10% of the total budget can be used for indirect institutional administrative costs.
- Up to $500 may be used to purchase any type of computer.
- Principal investigators are expected to use software available at the agency at which they are conducting the study (eg, workplace or school has SPSS license that PI can use).
- Include travel costs for ONE PI to attend the WOCN Society's annual conference to present findings. The total amount of grant budget should include the travel cost. Estimate $1200 to $1500.
- $500 will be withheld from your grant until an abstract reporting the study findings is submitted to the WOCN Society annual conference, and a manuscript of final results is submitted to CCI as a final report and to JWOCN for review for publication.
Budget Line Items
1. Supplies
(eg, camera, tape recorder) |
$ |
2. Photocopying
(eg, survey data forms, consent forms, etc.) |
$ |
3. Services
(eg, poster printing, data entry, etc.) |
$ |
4. Postage
(eg, to mail a survey) |
$ |
| 5. Consultants |
$ |
6. Research & Technical Support Staff
(statisticians, data entry) |
$ |
7. Computer-related
(eg, special software, laptop) |
$ |
8. Travel/Mileage
(to present findings, mileage to/from subject's homes) |
$ |
| 9. Other Costs |
$ |
10. Indirect Institutional Administrative Costs
(no greater than 10% of total) |
$ |
| TOTAL AMOUNT OF BUDGET REQUESTED: |
$ |
- BUDGET JUSTIFICATION. Please include a brief explanation of what each item is, why it costs, what it does, and indicate how each item relates to the research plan. The information should be sufficiently detailed to address cost and need.
- HUMAN SUBJECTS. If human subjects will be involved or medical record information of human subjects will be used, briefly explain the risks related to the study and how you will protect the safety and confidentiality of human subjects or their information. Indicate whether informed consent will be needed. If multiple institutions are data collection sites, address IRB approval at the various sites.
NOTE: Final approval of the study by an institutional review board/ethics committee is required after an award is made and before funds will be released.
- TIMELINE. Provide a timeline starting from submission of IRB proposal through data collection and analysis to submission of findings to WOCN Society annual conference and final report.
- SCIENTIFIC AND FUNDING OVERLAP. Explain if there is any overlap of the proposed project with other funds/grants received or pending by the principal investigator or study team:
- If your proposed study is contingent upon receiving a grant from another funding source, PI must explain which portion CCI will fund and which portion will be funded by the other funding source. CCI will take into consideration the ability to complete CCI portion of the grant independently from the other grant.
- If there is a majority or entire overlap of the grant submitted to CCI and another funding source and you are awarded funding by both, you must choose which grant you will accept.
- RECEIPT OF FUNDS. Please check below if the principal investigator or the employment institution will be accepting the funds:
- □ Principal investigator (If you choose this option, you will be required to include this as income on your income tax.)
- □ Employment institution
Name and complete mailing address of person/institution to whom funds will be sent:
- APPENDIX. The following materials are required or recommended in an Appendix:
- Letter of agreement to participate in study from institution in which the study will be conducted, or letter of agreement from Director of the clinical practice from which subjects will be recruited (required);
- Letter of agreement from consultants (required);
- Letter of support from a research mentor on the project, if applicable (required);
- Data collection instruments that are not readily accessible in the public domain/literature (recommended);
- If the study has already been approved by an IRB, please include in the Appendix.
NOTE:
- By accepting this grant, I agree to the terms of the Grant Award as outlined in the Research Grant Terms of Agreement.
- CHECKLIST
- All sections of the grant proposal must be completed in the final grant submission.
- Use this checklist to determine if your grant proposal is complete.
- Please assemble your grant submission in the following order, and put an “X” in the box to indicate that the item is completed:
□ II. A. Title Page
□ II. B. Other Team Members Contact Information
□ III. B. Abstract
□ III. C. Scientific Plan
□ III. D. Biosketch of Principal Investigator/Co-PI
□ III. E. Coinvestigator(s) Bio-sketch
□ III. F. Statement of Team Qualifications/Strengths
□ III. G. Project Budget
□ III. H. Budget Justification
□ III. I. Human Subjects
□ III. J. Timeline
□ III. K. Scientific and Funding Overlap
□ III. L. Receipt of Funds
□ III. M. Appendix
□ I have reviewed the “Research Grant Terms of Agreement” and agree to its terms if funded.
Questions?
If you have questions about your proposal submission, please contact Linda Dahle at [email protected] or 612.625.8159. If you have any scientific questions, please contact Dr. Donna Bliss, Director of the Center for Clinical Investigation, at: [email protected].
Appendix U: Web Sites for Evidence-Based Resources
ACP Journal Club
http://acpjc.acponline.org
Agency for Healthcare Research and Quality
http://www.ahcpr.gov/clinic/epcix.htm
Agency for Health Care Research and Quality (AHRQ): Quality and Patient Safety
http://www.ahrq.gov/qual/index.html
AHRQ Research Funding Opportunities
http://www.ahrq.gov/fund
American Academy of Nutrition and Dietetics
http://www.eatright.org
American Diabetes Association
http://www.diabetes.org
American Podiatric Medical Association
http://www.apma.org
American Society of Pain Educators
http://www.paineducators.org
Campbell Collaboration∗
http://www.campbellcollaboration.org
∗Site requires registration or a subscription through OVID or a similar service.
Canadian Centre for Health Evidence
http://www.cche.net
Centre for Evidence Based Medicine
http://www.cebm.net
Center for Gerontology and Healthcare Research
http://www.chcr.brown.edu
Centre for Reviews and Dissemination
http://www.york.ac.uk/inst/crd
Essential Evidence Plus
http://www.essentialevidenceplus.com
Implementing Best Practice Gateway
http://www.nursingsociety.org/Education/Pages/NewIBPKnowledgeGateway.aspx
Institute for Health Care Improvement (IHI)
http://www.ihi.org
Institute for Health Care Research and Policy (Georgetown Public Policy Institute)
http://ihcrp.georgetown.edu
Joanna Briggs Institute
http://www.joannabriggs.edu.au/Home
National Association for Continence
http://www.nafc.org
National Guidelines Clearinghouse
http://www.guideline.gov
National Institute for Clinical Excellence
http://www.nice.org.uk
National Pressure Ulcer Advisory Panel
http://www.npuap.org
Registered Nurse Association of Ontario
http://www.rnao.ca/bpg
Sigma Theta Tau International
http://www.nursingsociety.org/default.aspx
Society of Urological Nurses and Associates
http://www.suna.org
The Urology Care Foundation
http://www.urologyhealth.org
United Ostomy Associations of America, Inc
http://www.ostomy.org
University of Texas Health Sciences School of Nursing Academic Center for Evidence Based Practice
http://www.acestar.uthscsa.edu/index.asp
US Preventive Services Task Force
http://www.uspreventiveservicestaskforce.org/uspstf09/epbnursep/epbnursep.htm
Virginia Henderson International Nursing Library
http://www.nursinglibrary.org/vhl
WOCN Society
http://www.wocn.org/?page=research_funding
Searchable Databases
Cochrane Collaboration
http://www.cochrane.org
Cumulative Index of Nursing and Allied Health Literature
http://www.ebscohost.com/academic/cinahl-plus-with-full-text
EMBASE
http://www.embase.com
MEDLINE
http://www.ncbi.nlm.nih.gov/pubmed
PsycINFO
http://www.apa.org/index.aspx
PubMed
http://www.pubmedcentral.nih.gov
Government Resources
Centers for Disease Control and Prevention
http://www.cdc.gov
National Institutes of Health
http://www.nih.gov
US Department of Health and Human Services
http://www.hrsa.gov
Appendix V: Wound, Ostomy and Continence Nurses Society™ Advocacy and Grassroots Toolkit
Influencing Public Policy: Strengthening the Voice of the Wound, Ostomy and Continence Nursing Community
Originated By:
Wound, Ostomy and Continence Nurses Society (WOCN) National Public Policy/Advocacy Committee
Date Completed:
February 15, 2012
Table of Contents
- Introduction
- WOCN Society Grassroots Toolkit for State Advocacy
- The Basics: Communicating Directly With Your Legislator
- Increasing Your Voice: Building a Relationship With Your Legislator
- About Congress: Resources to Help You Navigate the Legislative Process
Introduction
The future growth and vitality of wound, ostomy and continence (WOC) nursing is largely dependent on the ability of our professionals to influence key decisions made in our state and nation's capitols. These policy decisions are essential to preserving the future of our practices, our health care facilities, and the patient populations that we serve. To protect our field of nursing, we must develop and deliver effective messages from credible messengers to our elected officials about the quality of our patient care and its importance to the community. This is the essence of advocacy, which can be implemented on many levels and take many different forms.
This toolkit will present a variety of options for incorporating advocacy efforts into your operations, from simply establishing regular communications with your elected officials to the more advanced efforts entailed in developing a grasstops or grassroots program to strengthen your influence in Washington, District of Columbia, or in your state capitol. The WOCN Society has prepared this toolkit as a resource for its members to enhance their own, individual efforts at public policy/advocacy. The WOCN Society continues to conduct direct lobbying on Capitol Hill, provide advocacy support and training, and coordinate all of the Society's government relations activities.
WOCN Society Grassroots Toolkit for State Advocacy
It is important for WOCN Society members to recognize that to be an effective advocate for our profession, we need to become involved in every level of government, including state and local policy. While the bulk of this toolkit focuses on federal activities, state legislatures across the country are playing a bigger role in health care policy than ever before. Since the enactment of the “Affordable Care Act” in 2010, states have been given broader authority and responsibilities with regard to health care policy decisions. Going forward, states will be largely responsible for the expansion of Medicaid authority, granted in the Affordable Care Act, and the establishment of their state Health Insurance Exchanges. State legislators will be more involved in coverage and reimbursement decisions than in past years.
WOCN Society members must be engaged at a state level because we are the eyes and ears of our profession and our patients. Policy decisions often happen quickly at the state level and can be made without the input of all stakeholders if those stakeholders are not engaged in the process. So, how do you become engaged in the process at the state level? There are some simple steps that can be taken:
- Stay Alert. Try to read about the activities of your state legislature in the newspaper or on health policy blogs that might be available in your state.
- Engage Other Stakeholders. Reach out to patient group leaders in your state as well as the public policy representatives you might have at your institution and ask that you be kept involved and considered a resource on health policy decisions.
- Research. Two great resources are listed later that can help you become well informed about state policy and your state legislatures. The National Conference of State Legislatures (NCSL) has a wealth of information about state policy and state legislators and has a dedicated Health Policy section. In addition, Project Vote Smart can help you identify who your state legislators are and how to contact them.
- Reach Out. The WOCN Society encourages all of its members to reach out to their state representatives, just as they would with their federal representatives. Being engaged is the best way to protect both your profession and your patients.
The Basics: Communicating Directly With Your Legislator
Legislators are greatly influenced by what they know and what they hear—especially from the people they represent. By communicating with a state legislator or a member of Congress, you can have a profound impact on the government policies that most affect your practice and the field of wound, ostomy and continence nursing.
Your elected officials need to hear from you. They hear from constituents and special interest groups about many diverse issues ranging from education to transportation to foreign policy. They need to hear from the nursing community as well. Do not assume that they know all the facts about the important role that wound, ostomy and continence specialty nurses play in delivering patient care in your community. It is incumbent upon you to provide them with the information they need to fully understand and appreciate the vital role of WOC specialty nurses.
Remember that you also should communicate with legislators from around your state and not just the elected representative from the district in which your facility or institution is located. Legislators from neighboring districts need to know that your WOC specialty nursing practice is essential and impacts their constituents.
Suggested Steps
Send an introductory packet to your congressional delegation, especially new legislators.
The beginning of a new Congress is an ideal time to introduce (or reintroduce) wound, ostomy and continence nursing.
- If a new member of Congress was just elected from your state, send a congratulatory letter to the legislator.
- Send a letter of congratulations to those who were reelected.
- Use this mailing as an opportunity to provide key information about your practice/facility to legislators from your state.
Provide information, such as the WOCN Society's position statements, to educate or update legislators in your state about the important role WOC specialty nursing plays in your community.
Use this first mailing to develop or strengthen your relationship with the office.
- Follow up with a phone call to the legislator's office.
- Remind the staff to contact you as a resource for further information.
- Extend an invitation for a visit to your practice/facility.
Maintain regular contact with a legislator's office.
Keep your legislators informed about your practice and facility.
- Find opportunities to send positive articles and information about wound, ostomy and continence nursing (eg, press clips, success stories, WOCNews [the official WOCN Society newsletter]) at least a few times a year.
Communicate clearly about relevant legislation—do not assume that they know where you stand.
- Communicate if you are for or against a piece of legislation.
- Thank the legislator for supporting any relevant legislation.
Depending on the urgency of the situation, use one of the following methods of communications:
- Fax—Faxed letters are very effective as they are likely to be given to the legislative staff immediately.
- Letter writing—Use letters primarily to accompany information packets, articles, etc., because postal mail arrives very slowly to Capitol Hill offices.
- E-mail—E-mail is particularly effective if you communicate directly through a staff's individual e-mail address, or if you are mobilizing a large number of people through the legislator's Web site.
- Phone calls—Phone calls are very effective because they provide an opportunity to talk directly to the staff, which reinforces your relationship with the office.
Writing a Letter
Constituent letters are a common way of communicating with a legislator and an effective advocacy tool.
- A personal letter will get more attention than a form letter or preprinted postcard.
- Make sure you include your name and address. Some offices will not open a letter if it is not from his or her state.
- Fax the letter to your member's office. Mail takes a long time to arrive because of security concerns with mail sent through the postal service.
Your letter should be simple and direct.
- If possible, limit your letter to one page.
- State the purpose of your letter in the first paragraph, identifying a specific bill number, if applicable.
- Focus on one particular issue and request specific action from the legislator.
- Explain how the issue will affect your local community.
Letters should be addressed as follows:
To a Senator
The Honorable (Full Name)
United States Senate
(Room Number; Building Name) Senate Office Building
Washington, DC 20510
Dear Senator (Last Name):
To a Representative
The Honorable (Full Name)
House of Representatives
(Room Number; Building Name) House Office Building
Washington, DC 20515
Dear Representative (Last Name):
Sending an E-mail
E-mail is an easy way to communicate with a legislator or staff member.
- If possible, try to secure an e-mail address of a particular staff member (the health Legislative Aide or the District Office Director) and e-mail him or her directly. This is highly effective.
- All legislators have a Web page with a link to contact the legislator. While this is a very easy way to communicate, it is less effective unless you are mobilizing a large number of people. Remember, legislators receive thousands of e-mails a week, so one individual e-mail can get lost.
State key information in the subject line.
- As it is easy to erase e-mails, you want to communicate key information in the subject line.
- State that you are a constituent and reiterate the issue in the subject line (eg, “Your constituent writing about ________ legislation”).
Keep your message brief and to the point.
- Do not forget your name and address in the text.
- Embed your message in the text. Attachments should be for background information, fact sheets, or endorsements.
Finding your legislator's Web site and e-mail.
- You can find your legislator's e-mail address by visiting either the House or Senate Web sites (www.house.gov or www.senate.gov) and searching for or selecting your legislator's name.
Telephone Calls to an Office
Phone calls are effective in delivering information quickly and directly, especially on days of key votes.
- State your position and ask what position the elected official is taking.
- Be prepared to explain how the issue will affect your practice and the legislator's constituents.
Calling the District Office.
- While the District staff may be less influential in terms of legislation compared to the DC staff, they are more accessible to constituents.
- Establishing a good relationship with the District Director is a very effective way to influence policy because the District office staff is responsible for constituent services.
Calling the Washington, DC, Office.
- When you call the Washington, DC, office, ask to speak with the health legislative aide.
- Remind the aide that you are a constituent and how many people your practice/facility serves in the state.
- Try to develop a dialogue that will allow you to call back in the future. Encourage your congressional staff contact to call you as a resource for information.
Sample Phone Script. Reference the legislator's Web site for the Washington and District Office phone numbers. You can locate his or her Web site by going to www.house.gov for House members and www.senate.gov for Senators. You also can call the Capitol operator at (202) 224-3121 and they will direct you to your legislator's office.
Sample Letter to a Legislator on a Key Issue. Constituent letters are an extremely effective advocacy tool. Your letter should be simple and direct. Ideally, it should not be more than 1 page since short letters tend to have the greatest impact. It should address only 1 issue and you want to be very clear about your position and request. Print your letter on personal stationery, if possible.
The Honorable (First Name; Last Name)
US House of Representatives/Senate
Washington, DC 20515 (for House)/20510 (for Senate)
Sent via facsimile: (202) (fax number)
Dear Representative/Senator (Last Name):
Sincerely,
Tips for Writing a Letter to a Legislator
- Fax Your Letter
- In light of security concerns on Capitol Hill, send your letter by fax rather than through the postal service.
- Opening Paragraph
- Introduce yourself as a constituent and how you are connected to the district.
- Thank the legislator for any past support that is applicable.
- State the purpose for your contacting the legislator. If applicable, reference a specific bill number.
- State the Facts
- Back up your position with facts.
- Provide information showing the impact of legislation on your practice/facility or on the legislator's district and constituents.
- Explain Consequences
- Provide information on the impact of opposing your request.
- Explain the impact on your community.
- Ask for a Response
- Restate your position.
- Ask for a response.
- Close the Letter
- Be sure to provide your contact information.
- If applicable, include a professional or organizational affiliation so the legislator sees that you are connected to the larger community.
Common titles and job functions in a congressional office. Members of Congress rely on their staff to assist him or her during a term in office, so knowing and understanding the titles and roles of these staff members are critical to communicating effectively with Congress. These are some of the common staff members in a congressional office:
Administrative Assistant (AA) or Chief of Staff (CoS). The AA or CoS is usually a person in charge of overseeing office operations and supervising key staff, but most importantly, this person reports directly to the Member of Congress. The AA/CoS typically has responsibility for evaluating the political outcomes of various legislative proposals in the member's district or state and constituent requests.
Legislative Director. The Legislative Director is typically the staff member who monitors the legislative schedule according to the interests and committee assignments of the member, supervises legislative assistants, and makes recommendations to the CoS or the member based on the likely or expected outcomes of particular issues.
Legislative Assistant. A legislative assistant is usually a staff person with specific interest and expertise on a particular issue or a number of issues. There are typically several legislative assistants in a given member's office and they will usually vary based on the interests of the member and his or her constituency.
Press Secretary (Press Secy.) or Communications Director (Comm. Dir.). The responsibility of the Communications Director is to establish clear and open lines of communication between the member, their constituency, the media, and the public at large. This staff member must be able to effectively promote the views and positions of their member on specific issues to these parties as clearly and briefly as possible.
Personal Secretary. This secretary or scheduler is responsible for appropriating the member's time to accommodate the many demands on his or her time including congressional and constituent requests and staff requirements. These responsibilities may involve making travel arrangements, scheduling speaking engagements or visits to the district, or making appointments with the member.
Caseworker or Legislative Correspondent. This staff member typically deals with constituents' requests, addressed to the member or to a federal agency, and prepares replies to those requests for the member's signature. These staff people will also address or resolve constituents' concerns over the phone. There are usually several of these correspondents in any given congressional office.
Increasing Your Voice: Building a Relationship With Your Legislator
Over time, you will have a much greater impact on public policy by developing and sustaining relationships with your elected officials and their staff. As a starting point, it is important for legislators to be aware of your practice and the community that it serves. However, for you to affect their decision making, they must come to know you, your hospital and clinics, the people you serve, and the other community leaders who form the backbone of your support.
Keep in mind that you also want to develop relationships with legislators from around your state, not just your elected representative. Legislators from neighboring districts need to know that wound, ostomy and continence nurses are providing essential nursing care to their constituents—even if the actual practice is not located in their district.
People respond to people, and it is important to build personal relationships. These can be with legislators or with their key legislative staff. Building a relationship will take time and hard work, but if done well, it has the potential to yield significant results for the WOCN Society and our practice. Ideally, you will be able to involve your stakeholders and build upon their existing relationships with legislators. Here are just a few ideas to get you started.
Suggested Steps
Get to know the district staff.
Building relationships with the district office can prove to be very useful.
- The district staff is responsible for constituent services. They will, therefore, be interested in meeting with you and learning about you and your practice.
- Begin by asking the District Director to meet with you and other leaders from your practice at the district office.
Use the first meeting to cultivate a relationship.
- At the first meeting, provide the staff with an overview of the practice/facility and the patient population that it serves.
- Invite the District Director to visit your practice/facility for a tour to learn first-hand how the practice of wound, ostomy and continence nursing impacts your community.
- Once you have developed a personal relationship with the District Director, it will be much easier to call him or her about a key piece of legislation.
Arrange for a visit to your medical or research facility by your legislator.
A first-hand tour of your facility is the most effective way to educate an elected official.
- Invite elected officials to visit your practice/facility by sending a letter or fax. Ideally, each legislator from your area, including those from neighboring districts, should visit your facility once a year.
- Follow up with a phone call to the office, remembering that legislators are in the district offices during congressional recess and on most Mondays and Fridays.
Prepare for the visit with clear goals.
- Prepare for the visit by coordinating closely with the legislator's staff, and determining the length of the visit.
- Develop a very clear agenda, identifying exactly who the legislator will be meeting with, what departments you will be visiting, the message, press availability, and the purpose for each stop on the tour.
- Use the tour to demonstrate the needs of the practice/facility and not just the accomplishments; identify services that could be provided with additional funding.
- Identify your legislative request(s), if any.
- Prepare appropriate take-away materials for your elected official.
Encourage a tour of the entire facility, including clinics.
- Given the breadth and depth of many practices/facilities, consider inviting legislators to see one of your clinics or community centers (eg, rural site).
- A visit provides an opportunity to develop a personal relationship with the legislator and senior stakeholders of the practice.
- Include opportunities for the legislators to meet with board members or other senior stakeholders. The goal is not just to educate the legislator but to build a relationship between the legislator and your leadership.
Visit your elected officials in Washington, District of Columbia Ultimately, you will want to schedule a personal visit to your members of Congress in Washington, District of Columbia. Elected officials will take notice of your visit. Taking the time out of your schedule to travel to Washington, District of Columbia, sends a very clear message to your legislators about the importance you place on public policy matters. Plan your visit carefully by being clear about what you seek to accomplish and whom you want to meet.
- The best days to visit a legislator in Washington, District of Columbia, are Tuesday, Wednesday, and Thursday.
- Make your appointments in advance. Ideally, you should contact the member's scheduler to seek an appointment a few weeks in advance.
- Call or fax a written request for a meeting with the legislator and his or her staff. Remind them if you are a constituent and how many constituents are served by your facility.
- Remember that a meeting with a member's legislative staff can be as important and productive as a meeting with the legislator.
Prepare for the meeting. Be prepared to state your specific request. Develop 2 to 3 well-documented talking points reinforcing your message.
- Use data if applicable to support your points.
- Be prepared to explain how your legislator's constituents benefit from this issue.
- If multiple people will be attending the meeting, determine in advance each person's role.
Follow up to the meeting.
- Send a thank you for the meeting.
- Include any information the legislator asked for and provide additional information to reiterate your message.
- Continue to cultivate the relationship.
- If the legislator acts positively upon your request, make sure you thank him or her and, if possible, publicize his or her support within your local practice, hospital, or research facility.
- The WOCN Society also publicizes government relations meetings and activities in the Society's newsletter.
Invite a legislator to one of your meetings.
Inviting an elected official to speak at a special facility, practice or hospital meeting is an opportune way to enhance the relationship. Take advantage of relationships that any of your leadership or board members may have with the legislator in arranging for the visit.
- Prepare for the visit by developing a clear presentation about your practice/facility and the services they provide to the community.
- If possible, incorporate senior leadership into the presentation.
Thank legislators and staff for their interest and support.
Take the time to thank legislators and staff whether it is for a meeting or support of legislation.
- Be certain to express your appreciation to a legislator following a meeting, practice/facility visit, or any other personal contact.
- Use the thank you as a way to continue building the relationship and as an opportunity to follow up with additional materials on your facility or on a particular legislative issue.
Sample Meeting Request Letter to a Legislator
Meeting face-to-face with a legislator is an effective way to develop a relationship and to impress upon an elected official the importance that you place on particular issues. Your letter should be simple and direct about your request for a meeting. If you are proposing to meet in Washington, District of Columbia, or in the legislator's district, be clear as to the specific date and time you will be available to meet.
The Honorable (First Name; Last Name)
U.S. House of Representatives/Senate
Washington, DC 20515 (for House)/20510 (for Senate)
Sent via facsimile: (202) (fax number)
Dear Representative/Senator (Last Name):
On behalf of (your facility's name) in (your city), I am writing to request a brief meeting with you on (day and date) anytime between (specific hours of availability). Representatives from our community, including (reference types of stakeholders; eg, “nurses”) will be in Washington, District of Columbia, that day and would welcome the opportunity to talk to you about the essential role that wound, ostomy and continence specialty nurses play in the local community.
As you may know (your practice/facility's name) is a vital part of our community's health care delivery system. We provide quality, accessible health care to all segments of our community. (Insert information about your facility, including the number of patients you serve, the number of people you employ, and your areas of expertise in medicine.)
Thank you for considering our request for a meeting on (date). We would very much appreciate it if your scheduler would contact me (or name of your government relations director if signed by someone else) at (phone number) to schedule an appointment.
Sincerely,
Tips for Writing a Meeting Request Letter to a Legislator
- Fax your letter
- In the light of concerns on Capitol Hill, particularly since the anthrax scare, send your letter by fax rather than through the postal service.
- Open the letter
- State up front the purpose of your letter, which is to request a meeting with the legislator in his or her office.
- Indicate if other people will be joining you and what subject you want to discuss.
- Bold the sentence that specifies the proposed date and times for the meeting so that it stands out.
- Be sure to reference the day of the week and the date (e.g., “Wednesday, March 3, 2005”) and the specific times during which you will be available to meet (e.g., “between 10 a.m. and 12:30 p.m.”).
- Provide facts on your practice
- Provide some background information on your practice/facility highlighting its role in the community and the number of constituents served.
- Specify follow-up steps
- Request that the legislator's scheduler call you to schedule the meeting or indicate that you will be following up.
- Provide contact information so the scheduler can follow up or call with any questions.
- Close the letter
- The letter could be signed by you, your practice or hospital leadership.
- Be sure to provide the person's title.
Do's and Don'ts: Tips for Meeting Your Representatives
Meeting with your elected officials is often the most effective way of educating them on a public policy issue. A face-to-face meeting provides an excellent opportunity to convey and receive information and to develop relationships that will benefit your cause. You can simplify the process by following the tips and guidelines outlined later.
Before the meeting
- Request the meeting in writing and follow up by phone to confirm the date and time and who will be attending the meeting.
- If other people will be accompanying you to the meeting, decide in advance each person's role. Designate one person as the facilitator.
- Be clear about the purpose of the meeting and what you want to accomplish.
- Do your homework ahead of time; research the legislator's voting record and know whether he or she sits on any key committees that affect your issue. You should visit the member's Web site and search online for useful background information.
- Prepare materials to bring to the meeting both as “props” during your presentation and as a leave-behind for the legislator.
During the meeting
- Be sure to arrive on time and dress appropriately (business attire).
- All participants should introduce themselves and indicate their position with their institution, and be sure to specify that you are a constituent.
- Start the meeting by thanking the legislator for meeting with you and, when appropriate, for being supportive of your position on an issue.
- Present your issue in a clear and concise manner.
- Try to incorporate a personal reference or anecdote to make the issue more real to the legislator.
- Request specific action from your legislator (eg, support for, or opposition to, a specific bill; floor remarks; talking to leadership).
- Do not argue.
- Do not lecture.
- After presenting your position, listen to the Legislator or Legislative Aide.
- If you do not know the answer to a question, do not be afraid to say that you do not know and that you will follow up after the meeting.
- Thank the legislator or aide for his or her time.
- Give the legislator the leave-behind packet you prepared.
After the meeting
- Write a thank you letter to the legislator that summarizes your conversation and any commitments that were made.
- Follow up and provide any additional information that was requested or offered.
- Please notify the WOCN Society's Executive Director about the substance of your meeting if relevant to the WOCN Society's membership at large.
About Congress: Resources to Help You Navigate the Legislative Process
This section contains background information on the US Congress and the legislative process. Included are links to a variety of Web sites that will be useful to you in tracking the status of legislation and planning your advocacy activities in Washington, District of Columbia
For specific information about the WOCN Society's advocacy efforts and federal legislation affecting the field of nursing, visit the WOCN Society's Web site at: http://www.wocn.org and click on “About Us” and then click “Advocacy and Policy.”
Congressional Calendar
The US House of Representatives and the US Senate maintain their own calendars of legislative activity. To obtain the most current calendar produced by each legislative body, you can visit their respective Web sites:
Status of Legislation
You can track the status of a piece of legislation through an online service offered by the Library of Congress. This Web site offers you the option of searching by a bill number, if known, or by a word or phrase. You can also monitor committee action and floor votes by visiting:
Contacting Your Members of Congress
To obtain contact information for your Senator or Representative (ie, phone number, fax number, or e-mail address), you should access their Web site. The easiest way to get to a member's individual Web site is through the House or Senate sites:
Congressional Committees
Each House and Senate committee has its own Web site with more detailed information on committee action and the status of legislation under its jurisdiction. Among the committees you may want to monitor are the following:
House jurisdiction relating to health care.
- Committee on education and labor. This committee deals with a number of health care–related education and labor issues including the access to quality health care for working families, worker health and safety, programs and services for at-risk youth, child nutrition, and poverty programs.
- Committee on energy and commerce. This committee and its subcommittees address issues pertaining to public health, hospital construction, mental health and research, biomedical research and equipment, Medicaid and national health insurance, food and drug regulation, drug abuse, and toxic substances.
- Committee on ways and means. This committee and its subcommittee on health address bills and matters related to programs providing payments for health care, health delivery systems or health research, programs under the Social Security Act, and tax credit and deduction provisions of the Internal Revenue Code dealing with health insurance premiums and health care costs. Specific programs addressed by this committee include Medicare, Temporary Assistance for Needy Families Program (TANF) and Old-Age, Survivors & Disability Insurance.
Senate jurisdiction relating to health care.
- Special committee on aging. This special committee addresses matters pertaining to problems and opportunities of older people including health maintenance and issues to obtaining care and assistance.
- Committee on health, education, labor, and pensions (HELP). HELP addresses matters relating to education, labor, health and public welfare, aging, biomedical research and development, occupational safety and health, and public health.
- Committee on finance. This committee concerns itself with issues of taxation and revenue, as well as insular possessions. More specifically, related to the concern for taxation and revenue issues, this committee addresses and has jurisdiction over most programs authorized by the Social Security Act and other health programs financed by a specific tax or trust fund. This includes Medicare parts A through D, Medicaid, Children's Health Insurance Program (CHIP), TANF, Maternal & Child Health Title XX Social Services Block Grant Program, Old-Age, Survivors & Disability Insurance, and the Physician Payment Review Commission.
House of Representatives
Appropriations
www.house.gov/appropriations
(202) 225-2771
H-218 Capitol Building
Labor, Health and Human Services, Education, and Related Agencies Subcommittee
(202) 225-3508
2358 Rayburn House Office Building
Energy and Commerce
http://energycommerce.house.gov
(202) 225-2927
2125 Rayburn House Office Building
Health Subcommittee
(202) 225-2927
2125 Rayburn House Office Building
Ways and Means
http://waysandmeans.house.gov
(202) 225-3625
1102 Longworth House Office Building
Health Subcommittee
(202) 225-3943
1136 Longworth House Office Building
Senate
Appropriations
http://appropriations.senate.gov
(202) 224-7363
S-128 Capitol Building
Labor, Health and Human Services, and Education Subcommittee
(202) 224-7216
184 Dirksen Senate Office Building
Finance
http://finance.senate.gov
(202) 224-4515
219 Dirksen Senate Office Building
Health Care Subcommittee
(202) 224-4515
219 Dirksen Senate Office Building
Health, Education, Labor and Pensions
http://help.senate.gov
(202) 224-5375
428 Dirksen Senate Office Building
How a Bill Becomes a Law
For a quick review of the federal legislative process, visit the Web site below. This site will step you through the process beginning with the introduction of legislation by a member of Congress, the role of committees, floor action, and eventually the President's signature.
www.vote-smart.org/resource_govt101_02.php
Glossary of Legislative Terms
The vote-smart Web site also includes a brief glossary of basic legislative terms. For a more comprehensive listing, visit the following Web site: www.thecapitol.net/glossary
Relevant US Government Agencies
To fully follow the development of policy in our nation's capital, you may also want to contact or access the Web sites of several executive offices, including Cabinet departments and federal agencies. These offices play a role in developing legislative proposals, which the administration submits to Congress for consideration. Depending on the issue and the legislation being proposed, you may want to contact officials in these offices to discuss any concerns or recommendations.
The White House
www.whitehouse.gov
(202) 456-1414
1600 Pennsylvania Avenue, NW
Washington, DC 20500
US Department of Health and Human Services
www.dhhs.gov
(202) 690-7000
200 Independence Avenue, SW
Washington, DC 20201
Centers for Medicare & Medicaid Services
www.cms.hhs.gov
(410) 786-3000
4700 Silver Hill Road
Suitland, MD 20746
Food and Drug Administration
www.fda.gov
(301) 827-2410
5600 Fishers Lane
Rockville, MD 20857
National Institutes of Health
www.nih.gov
(301) 496-4000
9000 Rockville Pike
Bethesda, MD 20892
Office of Management and Budget
www.omb.gov
(202) 395-3080
725 17th Street, NW
Washington, DC 20503
Date Approved by the WOCN Society Board of Directors: March 20, 2012
Appendix W: Structure of Medicare and Medicaid in Relationship to the Rest of the Government Branches
How Medicare Policy Is Established

Appendix X: How Medicare Policy Is Implemented